BLACK WORLD NEWS
What matters to you, today
What matters to you, today
291 stories collected. Newest first.

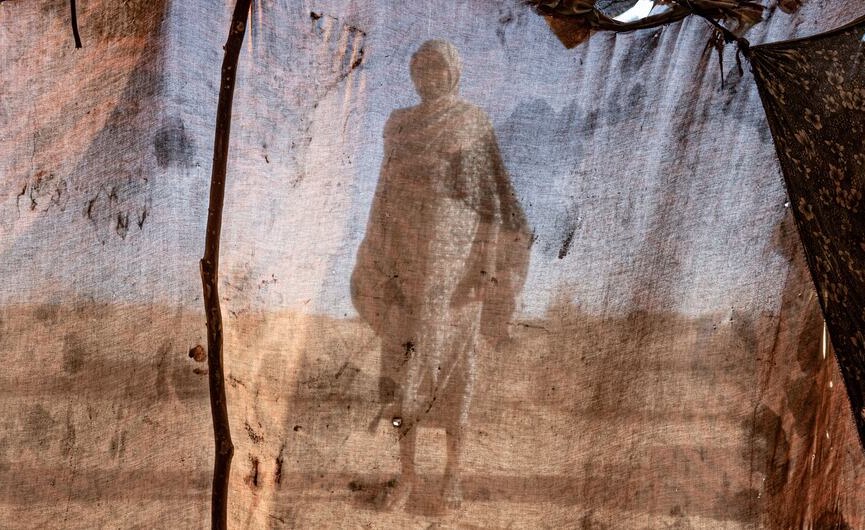
The article visualizes how conflict, aid cuts, and attacks on health workers are accelerating Ebola's spread in the Democratic Republic of Congo. It highlights armed group activity, displacement, and funding shortages as key drivers of the outbreak in Ituri, North Kivu, and South Kivu.
The Congolese appear mainly through infection counts and mortality figures, which reduces a complex humanitarian crisis to depersonalized data points.
Armed groups and militias controlling resource-rich territories.

The UN report details Somalia's severe humanitarian crisis driven by drought, conflict, and disease, with 7.5 million people affected. It highlights acute malnutrition, water shortages, and a strained health system, but focuses on needs rather than systemic causes.
Portrayed as passive victims of drought and disease, Somali communities appear solely through crisis statistics, erasing their agency and resilience.
International food and water corporations profit from inflated prices.

Somalia faces severe humanitarian crises from drought, conflict, and disease outbreaks, with 4.4 million people in acute food insecurity and 1.85 million children malnourished. Displacement, protection risks, and funding shortfalls exacerbate the situation, though a narrower scope for 2026 reduces the official needy count.
Black Somalis emerge as passive victims of climate and conflict, their suffering quantified into alarming numbers that obscure systemic neglect.
International aid organizations and their contractors benefit from sustained crisis funding.

A Bangor University study finds that deindustrialization in Wales, particularly coal mining's decline, has caused long-term poor mental health, especially among those who lived through it. The research links historical mining data to large health surveys, showing that women are as affected as men. Policymakers are urged to mitigate such health costs during future economic transitions.
Welsh mining communities, including the few Black residents, appear as casualties of industrial collapse, their mental suffering reduced to a historical statistic.
Coal mining corporations and the UK government.

The report uses Afrobarometer survey data to show widespread drug abuse in Zimbabwe, particularly among youth, and notes government plans to address it. It frames the issue as a public health and law enforcement challenge, while implying unemployment and economic crisis contribute to the problem.
Statistics stand in for people when the report quantifies Zimbabweans' suffering through admission rates and survey percentages, reducing a community crisis to data points without exploring underlying systemic drivers.
The pharmaceutical and rehabilitation industries benefit from increased addiction-related profits.

This article offers advice for partners of alcoholics, focusing on individual behavior change. It lacks any mention of systemic racism or the disproportionate impact of alcohol addiction on Black communities. The framing implies addiction is a personal failing rather than a product of structural inequality.
The article reduces alcoholism to a generic personal problem, ignoring how structural inequalities and targeted alcohol marketing devastate Black communities.
Alcohol industry profits from targeted marketing in Black neighborhoods.

The article explains the neurological mechanisms behind alcohol addiction and promotes a Nashville-based rehab center. It focuses on individual biology and treatment options without addressing broader social or racial inequities.
Readers encounter alcohol addiction as a clinical brain disorder, stripped of any racial context, which obscures the systemic barriers Black communities face in accessing treatment.
Alcohol industry and treatment centers gain financially.

A food security program in Chocó reduced child malnutrition and diarrhoea among Afro-Colombian and indigenous communities. The region is rich in natural resources but suffers from extreme poverty, low life expectancy, and violence over resource control.
Communities are reduced to statistical measures of malnutrition and poverty, implying their suffering is a technical problem rather than a human crisis linked to systemic resource extraction.
The mining industry benefits most from the conditions described.

Germany reports a record high in drug-related deaths, with a sharp increase among under-30s linked to synthetic opioids and polydrug use. The report focuses on general data and dealer marketing tactics but does not address race or structural inequality affecting Black communities.
Statistics stand in for people when the article presents rising death counts without any reference to Black communities or racial disparities in drug-related mortality.
Pharmaceutical and synthetic opioid producers benefit from the ongoing crisis.

The article describes alcohol use disorder as a chronic disease with signs, risks, and treatment options. It does not address racial disparities or structural factors affecting Black communities.
Nearly 30 million people are reduced to a number, stripping Black communities of context and masking the systemic roots of alcohol addiction.
Alcohol industry profits from targeted marketing.

The study finds Black populations have higher overall prescription drug use but lower rates per prevalent condition compared to the all-population average, indicating undertreatment relative to disease burden. This reveals racial disparities in healthcare access and quality.
Black patients become data points showing lower prescriptions relative to disease burden, implying systemic undertreatment rather than individual need.
Pharmaceutical insurers and drug pricing intermediaries benefit most.

Thousands of mental health crisis patients in England wait up to three days in A&E for a bed, with conditions described as 'close to torture.' The Royal College of Nursing reports that delayed admissions have skyrocketed since 2019, while mental health beds have been cut and staffing lags behind demand.
The article reduces Black communities to faceless numbers in a mental health crisis, implying systemic neglect and dehumanization without naming race explicitly.
The UK government and NHS trusts benefit from underfunding mental health services.
This market research report analyzes the growth of the youth mental health crisis intervention platform industry, highlighting its projected increase from $3.68 billion to $14.16 billion. While noting rising rates of anxiety and depression, it omits any discussion of how structural racism or economic inequality disproportionately affects Black youth access to care.
Black youth are reduced to a market opportunity and data point, with their rising mental health needs framed as a growth sector for tech investors rather than a systemic crisis requiring structural change.
Private platform developers and AI crisis intervention companies.

Child mental health referrals in England have surpassed one million, with anxiety and neurodevelopmental conditions driving the rise. Black children are underrepresented in referrals and far more likely to be in crisis when finally seen, highlighting racial disparities in access to early support.
Black British children are depicted largely as a data point showing delayed referrals, entering mental health services only in crisis, which reveals systemic neglect.
The National Health Service reduces costs by limiting early intervention.

The page is a geolocation popup for The Recovery Village, a for-profit drug and alcohol treatment provider. It lists services across multiple U.S. states but contains no specific news story, only promotional content for addiction treatment.
Black communities are portrayed as passive consumers of addiction treatment services, with their struggles commodified by a for-profit rehab network.
The Recovery Village, a for-profit treatment chain.
A new cholera outbreak in war-torn Sudan has killed over 100 people, with cases concentrated in Darfur and Kordofan. The WHO warns that the disease will worsen as rains begin, amid ongoing conflict and limited aid access.
The people of Sudan appear primarily as vulnerable victims of war and disease, their suffering framed as a humanitarian crisis needing foreign intervention.
The article warns that delayed containment of the Ebola outbreak in DRC and Uganda could cost billions and cause thousands of additional deaths. It emphasizes the need for significant health financing to prevent a wider crisis.
Black communities are reduced to mortality projections and economic costs, with the human dimension of suffering obscured by quantitative modeling.
International health organizations and donor governments benefit from containment narratives.

An epidemic coalition in the Democratic Republic of Congo is focusing on deploying an Ebola vaccine specifically tailored to the Bundibugyo strain. This collaborative effort involves local health authorities and international partners to contain outbreaks in vulnerable communities.
Black Congolese communities emerge as active participants in public health efforts, challenging stereotypes of passivity by driving a coalition-focused Ebola vaccination campaign.
International pharmaceutical companies gain through vaccine trials and distribution contracts.

The Ebola outbreak in DR Congo has surpassed 500 deaths, with no vaccine or treatment for the Bundibugyo virus. Health workers threaten strike action over low wages and poor conditions, while armed conflict hampers response efforts.
The coverage reduces Black Congolese communities to death counts and infection tallies, erasing their humanity and the systemic neglect driving the crisis.
The Congolese government and international health agencies benefit from underfunded response structures.

The Africa CDC and WHO report that the Ebola outbreak in DR Congo and Uganda is outpacing containment efforts, with rising cases and deaths. Despite some progress in testing and treatment, insecurity and limited resources hinder the response, risking regional economic losses.
The coverage reduces Congolese lives to case counts and death tolls, portraying the outbreak as a logistical problem rather than a human tragedy.
Global pharmaceutical companies benefit from vaccine trial opportunities.

The Democratic Republic of the Congo has confirmed 600 Ebola deaths amid a worsening outbreak. Healthcare workers in Ituri province are walking off the job over unpaid wages and limited supplies, as clinical trials for the Bundibugyo virus begin.
Healthcare workers appear as exploited laborers risking their lives without pay, while Black communities are reduced to infection numbers and a backdrop for clinical trials.
International pharmaceutical companies seeking trial data.

The Trump administration is offering healthcare aid to African nations but with conditions that prioritize U.S. pharmaceutical companies. Some African governments resist these deals, viewing them as unfair and transactional rather than cooperative.
African nations are depicted as bargaining partners whose health systems must bow to U.S. commercial interests, implying their autonomy is secondary to American profit.
U.S. pharmaceutical and medical firms.

The article reports on global backlash against the collapse of USAID under the Trump and Musk administration, linking the cuts to a Lancet study projecting 14 million deaths. It highlights how the dismantling of aid disproportionately harms Black communities in the Global South who rely on these programs for healthcare and survival.
Black and African communities are reduced to a death toll in the Lancet study, their suffering obscured by a numerical headline.
Privatized healthcare and aid corporations who benefit from dismantling public systems.

In eastern Democratic Republic of Congo, Ebola misinformation fuels attacks on health workers, including assaults and arson at treatment centers. The violence is tied to false claims that Ebola is not real or that responders are scheming for money.
The story frames Black communities in the DRC as resistant to science and prone to violence, implying that their distrust is baseless and self-destructive.
International health organizations and pharmaceutical companies benefit from undisturbed outbreak response.

The Africa CDC reports that the current Ebola outbreak is the fastest growing ever recorded. The story focuses on the speed and scale of the outbreak, but does not address deeper systemic issues.
The outbreak is presented as a rapidly growing numerical crisis, with little mention of the underlying systemic factors affecting Black communities in affected regions.

The article discusses Nigeria's shift from donor-funded nutrition programs to domestic financing, arguing that malnutrition reflects institutional coordination failures. It links nutrition to broader governance and national security challenges.
The piece frames Nigerians as passive recipients of donor aid, reduced to a funding gap and coordination problem rather than people with agency.
The Nigerian government and political elites benefit most.

The piece examines how media misinterpreted a UN maternal mortality report, implying a worsening crisis in Nigeria without contextualizing the data as pre-reform. It highlights the importance of accurate framing to avoid misleading the public about ongoing health interventions.
The article critiques how outdated maternal mortality statistics are presented as fresh crises, reducing Nigerian women to numbers that obscure ongoing government and international reform efforts.
International media outlets benefit from sensationalized headlines driving engagement.

Barbados' Chief Medical Officer confirms no new cases of scarlet fever, chicken pox, or monkeypox, attributing previous school cases to community and family clusters. He reassures the public, emphasizes sanitation and respiratory etiquette, and urges reporting of symptoms to general practitioners.
Black Barbadian families are portrayed as concerned caregivers, with public health officials openly addressing their fears and providing clear, non-alarmist information.
The Barbados Ministry of Health and Wellness.

Queen Elizabeth Hospital in Barbados plans to dispose of 65 unclaimed bodies under new regulations. The story highlights the financial cost of storage but offers little context on the systemic factors that may lead to bodies going unclaimed in a predominantly Black nation.
The coverage reduces deceased Black Barbadians to a financial burden and a list of names, implying their lives lacked community or familial value.
The Queen Elizabeth Hospital and the Barbados government benefit from reduced storage costs.

An Ebola treatment trial begins in the Democratic Republic of Congo, targeting the less common Bundibugyo strain. More than 1,400 people have been diagnosed and 438 have died in the outbreak.
By highlighting the urgency and hope of the treatment trial, the story portrays Congolese communities as actively struggling against disease rather than passive victims.
Global pharmaceutical companies and international health organizations.

A person in Scotland tested negative for Ebola, amid an outbreak in central Africa that has killed over 360. The story focuses on the UK's precautionary measures while treating the African outbreak as a distant statistic.
The story presents African nations merely as a backdrop of rising Ebola cases, reducing a humanitarian crisis to a numbers update without portraying affected communities as people.
Global health surveillance systems and Western public health agencies.

Nueva EPS, a major Colombian health insurer, reveals a $22 billion peso debt, with the state acknowledging half the liability. Users face systematic delays in procedures and medication, highlighting a healthcare system in crisis.
Black and Afro-Colombian users are reduced to passive casualties of a financial disaster, their suffering from delayed care and denied medicines rendered invisible behind corporate debt figures.
Private healthcare providers and the Nueva EPS corporate structure.

The Ebola outbreak in DR Congo is described as the fastest growing ever, with cases doubling every 28 days and 600 confirmed deaths. Health officials warn the virus is outpacing response efforts and billions of dollars are needed.
This report reduces Congolese lives to doubling rates and death tolls, erasing the human dimension of the outbreak.
Pharmaceutical corporations and global health bodies benefit from emergency funding and vaccine contracts.

The Democratic Republic of Congo faces a resurgence of Ebola with over a thousand confirmed cases, particularly concerning as the virus spreads to urban areas. Experts highlight population mobility and fragile health systems as key drivers, while authorities ramp up surveillance and awareness campaigns.
The coverage reduces Congolese lives to infection numbers and logistical hurdles, implying their suffering is a problem to be managed rather than a human crisis.
International pharmaceutical and response organizations gain contracts and influence.

The story details how nearly two million Somali children face acute malnutrition due to drought, conflict, and funding shortages. It highlights the closing of health facilities and the impact of the Middle East war on supply chains, but does not examine deeper colonial or economic exploitation.
The children and families appear as passive victims of intertwined climate shocks and distant conflicts, their suffering reduced to a humanitarian statistic without addressing root causes.
Global fuel and shipping corporations benefiting from supply chain disruptions.

Verywell Mind's article on alcohol and substance addiction offers a general overview of causes, symptoms, and treatments. It does not address how structural racism or economic exploitation shape addiction patterns or access to care for Black communities.
The content presents addiction as a medicalized condition devoid of racial context, erasing the specific ways Black communities face disproportionate barriers to treatment.
Pharmaceutical and rehab industries benefit from universalizing addiction without addressing systemic inequities.

Alcoholics Anonymous promotes its peer-support program as free and open to all. The content does not mention race or structural inequality, but the framing assumes equal access that Black communities do not have due to historical and economic barriers.
The story presents a universal recovery program without racial markers, but Black communities face unique barriers to access that remain unaddressed.
Alcoholics Anonymous as an organization benefits from the portrayal.

Three studies reveal that patients with limited English proficiency in the US, ethnic minorities in European psychiatric settings, and Black patients in the UK face higher rates of physical and chemical restraint due to language barriers, structural inequality, and institutional racism. The research highlights how clinical decision-making is biased by credibility gaps and unconscious racism, leading to disproportionate harm.
Patients with limited English proficiency are reduced to data points, their higher rates of restraint and sedation presented as clinical outcomes rather than human rights violations.
Hospitals and pharmaceutical companies benefit from chemical restraint practices.

Alcoholics Anonymous Great Britain presents its 2025 survey as a success, focusing on fellowship and trends without mentioning race. This omission erases how structural inequality and alcohol industry targeting disproportionately affect Black communities.
The page reduces recovery to survey trends, making Black communities invisible in a fellowship where access barriers and historical mistrust remain unacknowledged.
Alcohol industry profits from unaddressed disparities in treatment access.

The article fails to address how systemic racism and economic exploitation cause higher COVID-19 rates in Black communities. Instead, it mixes unrelated medical content, reflecting how Black health crises are often deprioritized.
Black Americans appear here mainly as a statistical category hit hard by COVID-19, stripped of their human experiences beyond the infection numbers.
Healthcare systems and insurers benefit from framing the crisis as data-driven rather than structural.

The article describes a Brazilian Ministry of Health initiative to strengthen public health emergency preparedness across all 27 federative units. It focuses on training and action plans but does not address racial disparities in health outcomes.
Black Brazilians are largely invisible in this technical piece about health system capacity, their structural vulnerabilities subsumed under neutral, quantitative language about emergency preparedness.
Brazil's Ministry of Health and the Unified Health System (SUS).

Dr. Alvin Thomas warns of a mental health crisis in the Black community, especially among men and boys, due to COVID-19 and police violence. He argues that systemic racial injustice must be addressed through policy changes and societal recalibration. The piece offers resources and ends with cautious optimism.
Black men and boys are portrayed as facing a looming mental health crisis, cast as victims of converging systemic violence and pandemic trauma.
University of Wisconsin–Madison benefits from research funding and institutional visibility.

The article highlights that Black adults are significantly less likely than white adults to have received mental health services in the past three years, despite reporting similar or worse mental health. This disparity points to ongoing structural barriers in healthcare access for Black communities.
Black adults are reduced to a single percentage gap in service usage, implying their mental health struggles are a matter of access rather than systemic neglect.
Private mental health insurers and providers who profit from selective access.

This article tells the story of Ann, a Black mother in Baltimore whose untreated schizophrenia led to addiction and family separation. It argues that mental health issues in Black communities are rooted in poverty, trauma, and systemic neglect, and proposes a culturally competent, home-based treatment model.
Black Americans appear here mainly as individuals trapped in cycles of trauma and self-medication, their struggles framed as systemic failures requiring holistic care.
Pharmaceutical companies and private insurance firms benefit from inadequate public mental health funding.

The article argues that liberal ideology, including feminism and independence, is driving a mental health crisis among Black women, citing lower marriage rates and higher depression. It ignores systemic factors like economic inequality and racism, instead framing the issue as a cultural or ideological failure.
Black women are reduced to a set of alarming statistics implying their mental health crisis stems from embracing liberal values rather than structural racism.
Conservative political groups and media that benefit from framing liberal ideology as harmful.

The Ebola outbreak in eastern DRC is worsened by a humanitarian crisis, with conflict and displacement hindering access to camps. Health workers face skepticism from communities that lack basic services, demanding a broader response beyond Ebola.
The communities are reduced to numbers and obstacles, their deep mistrust framed as a logistical problem rather than a response to historical neglect.
International pharmaceutical and health logistics corporations.

Persistent glitches in Kenya's Social Health Authority system have disrupted hospital services for a week, forcing a return to slow manual processes. The technical failures delay patient care and highlight systemic vulnerabilities in the country's digital health infrastructure.
Patients are depicted as passive victims of a malfunctioning state system, their health compromised by technical failures that reveal deeper neglect.
The Digital Health Agency and technology contractors benefit from system contracts.

A newly built mother and child hospital in Akwa Ibom, Nigeria, remains locked months after its commissioning, leaving women like Blessing Okon to suffer complications during childbirth. The facility's idleness reflects systemic failures in healthcare infrastructure that disproportionately harm Black women.
By centering the story on a woman's agonizing labor and complications, the article portrays Black women as victims of failed state infrastructure rather than agents of their own care.
Akwa Ibom State government officials who commissioned the hospital but left it idle.

BBC Radio DJ Trevor Nelson MBE announces he is taking a break from work to address health issues after routine check-ups. Colleagues and fans express support, wishing him a speedy recovery. The nature of his condition remains undisclosed.
Portrayed with dignity and support, this story presents a Black media figure simply as a person facing health challenges, avoiding racial stereotypes or pathologization.

Tamara and Damion Thomas were jailed for gross negligence manslaughter and neglect after delaying medical care for their 12-year-old son Joshua, who died of diabetic ketoacidosis. The story focuses on their failure to seek timely help, without addressing broader systemic issues in healthcare access for Black families.
The parents are portrayed as negligent and blameworthy, reinforcing harmful stereotypes about Black familial care and responsibility within the healthcare system.
The state benefits by deflecting attention from systemic healthcare failures onto individual parents.

France confirmed an Ebola case in a doctor returning from DR Congo, where a Bundibugyo virus outbreak has killed 277. The story emphasizes France's containment capacity while reducing the Congolese outbreak to case counts.
The coverage reduces Congolese people to a tally of 1,094 cases and 277 deaths, stripping their crisis of human context and portraying them as passive infection vectors.
France benefits by reinforcing its medical superiority narrative through the containment of a single case.

The WHO announced a clinical trial for two Ebola drugs in the Democratic Republic of Congo, as the outbreak continues. The trial evaluates MBP134 and remdesivir for treating the Bundibugyo virus strain, involving local and international partners.
The story presents Black communities primarily through the lens of international health collaboration and scientific progress, though local voices are notably absent.
WHO and Gilead Sciences benefit from testing and funding of new Ebola treatments.
The article reports on the Ebola epidemic in the DRC, emphasizing that declining case numbers reflect failed surveillance, not containment. It highlights how local communities view Ebola as a lesser threat than the violence and poverty caused by imperialist exploitation.
Communities are shown as victims of structural neglect, more threatened by imperialist conflict and poverty than Ebola, highlighting systemic abandonment.
Western pharmaceutical and extraction industries benefit from the region's instability.

The article reports on the Ebola outbreak in a displacement camp in Bunia, DRC, where basic needs like water are scarce. It emphasizes the daily struggle of displaced people against the disease amid inadequate resources.
Portrayed as victims of a cascading crisis, displaced Congolese face Ebola with scarce water, highlighting systemic neglect rooted in colonial-era infrastructure deficits.
International pharmaceutical companies benefit from Ebola vaccine contracts.

The article compares American and French framing of crack cocaine use, finding that in the U.S., the drug is portrayed as a Black urban problem, which widens racial health gaps. France's framing is different, focusing more on public health.
Black Americans in this study are shown as scapegoats for crack cocaine, with media bias worsening their health disparities.
American media and pharmaceutical industries.

The article presents UK alcohol addiction statistics and causes, focusing on mental health, social norms, and regional trends. It does not address how structural racism or industry targeting affects Black communities differently.
Black Britons are rendered invisible in this story, as the data aggregates all racial groups, masking how alcohol industry targeting and unequal access to treatment disproportionately harm Black communities.
Alcohol industry and its shareholders.

This UK government report updates alcohol statistics for England, showing rising hospital admission rates. However, it does not break down data by ethnicity, erasing how structural inequality and targeted marketing may disproportionately affect Black communities.
Black communities are invisible in this data-driven report, their specific experiences drowned out by aggregate numbers that obscure racial disparities.
The alcohol industry benefits from normalized consumption patterns across all demographics.

ASAM releases a three-part policy series examining systemic racism as a social determinant of health affecting BIPOC with substance use disorder. The statements recommend trauma-informed care, addressing social determinants, and decriminalizing drug possession to achieve racial justice.
Black communities are shown as facing compounded harm from systemic racism in addiction care, which positions them as deserving of trauma-informed, equitable treatment.
Healthcare systems and addiction medicine professionals benefit from the proposed reforms.

This article highlights Black Mental Health Week in Canada, which aims to address mental health inequities rooted in anti-Black racism and historical trauma. It discusses a CAMH art exhibit showcasing Black youth works and the generational stigma linked to slavery.
Readers meet these communities as people actively fighting stigma by sharing personal stories and art, highlighting resilience and the need for systemic change.

A new report highlights that mental health is the most common chronic condition among Black women in Canada. Clinicians and patients attribute this to the compounding effects of anti-Black racism and misogyny, revealing a systemic crisis in healthcare access and support.
Black women are presented as a diagnosed category, their suffering quantified into a chronic condition that underscores systemic neglect.
The Canadian healthcare system, which shifts blame onto patients rather than addressing roots.

The article highlights research showing that father absence contributes to depression, anxiety, and rising suicide rates among Black youth in Canada. It frames the issue as a mental health crisis requiring targeted support and intervention.
Black youth appear here as casualties of father absence, with their mental health struggles reduced to statistical evidence rather than explored through systemic racism and colonial family disruption.

The requested page is blocked by a security service, so no story content is available. The title suggests it would present alcohol and drug abuse statistics, likely without racial or historical context.
The inaccessible page reduces addiction to decontextualized numbers, erasing the historical and structural forces driving substance use in Black communities.
Unclear, as the content is blocked.

DR Congo announces free healthcare for all illnesses in Ituri as Ebola resurfaces. The move aims to contain the outbreak and address long-standing health access gaps in the conflict-affected region.
The residents of Ituri emerge as people deserving care in a moment of crisis, but their ongoing suffering from a neglected colonial legacy is only hinted at.

The closure of the Goma-Gisenyi border after an Ebola case in Goma has devastated the livelihoods of thousands of small-scale traders. Health officials defend the restrictions, but critics argue surveillance would be more effective and less harmful.
The story presents Black traders as economic casualties of a health crisis, reducing their lives to numbers and disrupted routines while Rwanda's border policy exploits their vulnerability.
Rwandan health authorities and border control benefit from the closures.

The DR Congo government introduces free healthcare in Ituri province to combat an Ebola outbreak exceeding 1,000 cases. The pilot project aims for nationwide expansion, while WHO warns the outbreak remains serious.
Congolese communities emerge as proactive agents in this story, capable of mobilizing free healthcare and containment measures despite systemic neglect.
The Congolese government gains legitimacy and international goodwill.

Kenya's health minister was held in contempt for defying a court order to stop building a US-funded Ebola quarantine center. The facility, intended for American citizens, has sparked deadly protests and legal challenges over public health risks and sovereignty.
Kenyans appear as subjects of a US-driven health security agenda, with their protests and deaths reduced to obstacles to a foreign facility.
United States government and its biosecurity interests.

A senior doctor in Benue State, Nigeria, died from Lassa fever amid a fresh outbreak. The health commissioner confirmed the death and noted the state was near declaring the outbreak over before this case emerged.
A doctor's death is reported as a statistic within a broader outbreak, overlooking the systemic neglect of rural healthcare infrastructure that endangers Black lives.
The Nigerian government benefits from underfunded rural health systems.

MSF has suspended services at the Isaïe Jeanty Maternity Hospital in Haiti due to escalating armed violence, leaving thousands of women without maternal healthcare. The facility, in Cité Soleil, was caught in crossfire, forcing staff to evacuate and patients to seek unsafe home births.
Haitian women emerge as vulnerable yet resilient figures, their lives endangered by violence that renders medical care inaccessible, highlighting systemic neglect.
Armed groups benefit from the chaos that destabilizes state infrastructure.

A woman in Barbados is suing the government over alleged injuries from the AstraZeneca COVID-19 vaccine. She claims the vaccine was defective and that the government failed to provide adequate compensation mechanisms for adverse reactions.
The plaintiff in this lawsuit is portrayed as a victim of a defective vaccine and government negligence, highlighting systemic failures in post-colonial healthcare accountability.
The pharmaceutical industry benefits from limited liability frameworks in vaccine programs.

A woman in Barbados has sued the government over severe health complications after receiving the AstraZeneca COVID-19 vaccine, alleging the product was defective. Her case underscores potential medical negligence and lack of government response.
The woman appears as a victim of a state-mandated vaccine, highlighting systemic failures in medical safety and government accountability.
AstraZeneca, as the vaccine manufacturer, benefits from limited liability.

The article explains the chemical mechanisms behind alcohol addiction, focusing on dopamine release and neurotransmitter disruption. It presents addiction as a universal brain-based condition without reference to specific populations or structural inequalities.
Alcohol addiction is discussed purely in chemical and neurological terms, removing any social context or human experience from the equation.
The alcohol industry.

This article explains the physical and psychological mechanisms behind alcohol addiction, citing national statistics on youth drinking and binge drinking. It does not address how alcohol marketing, economic exploitation, or historical trauma disproportionately affect Black communities.
Readers encounter Black communities largely as numbers in a national survey, stripped of context about the targeted marketing and structural stressors that drive addiction rates.
Alcohol industry profits from continued consumption and addiction.

The study finds that rising inflation and Bank Rates in the UK cost-of-living crisis correlate with increased discrimination and worsening general and mental health for Black people. This reveals how macroeconomic policy exacerbates racial health disparities.
Black individuals are depicted as bearing the disproportionate health burden of economic policies, their suffering reduced to a statistical correlation with inflation and interest rates.
The Bank of England and financial institutions benefit from interest rate policies.
/filters:format(webp)/filters:no_upscale()/prod01/cdn/media/stirling/news/news-centre/2025/apr-25/1200X630iStock-938718572.jpg)
A University of Stirling study reveals that the Norwegian Oil Fund invests in alcohol companies using marketing tactics in six African countries that are banned in Norway. These activities, including sports sponsorships and youth-focused promotions, exploit weaker regulations to maximize profits.
African communities emerge as passive targets of predatory alcohol marketing funded by a wealthy foreign pension fund, implying their health is expendable.
The Norwegian Oil Fund and alcohol corporations.

Cheryl Wisseh discusses the structural factors driving racial disparities in COVID-19 outcomes, including historical inequities and systemic neglect. She calls on pharmacies and health systems to address these root causes rather than just treating symptoms.
Black communities are presented through disparities data that obscure individual experiences, reducing systemic suffering to a measurable gap in outcomes.
Pharmaceutical and healthcare systems that profit from treating rather than preventing illness.

The article examines mental health challenges in Black communities, highlighting stigma, socioeconomic disparities, and discrimination as barriers to care. It notes that only one in three Black adults who need mental health treatment receives it, and that poverty and racism compound psychological distress.
Black Americans appear here mainly as statistical subjects whose mental health struggles are documented through disparities and unmet needs, implying systemic neglect.

The article promotes Treatment-Centers.net, a free referral service connecting individuals to drug and alcohol treatment centers. It emphasizes matching clients to the right facility and highlights the founder's personal recovery story without addressing racial disparities in treatment access.
Black people are invisible in this article; the generic addict is portrayed without race or context, erasing the systemic factors driving substance use disorders.
Private treatment referral services and for-profit rehabilitation centers.

A study shows the HPV vaccine has eliminated cervical cancer deaths among young women in the UK. However, the highest death rates remain in low-income countries, particularly in sub-Saharan Africa, highlighting global healthcare inequities.
Statistics dominate the coverage, reducing Black women globally to data points without addressing unequal access to vaccines and screening.
Pharmaceutical companies producing the HPV vaccine.

The US cuts $400 million in annual HIV funding to South Africa, citing unproven claims of anti-white racism. Over 8 million Black South Africans face disrupted antiretroviral care as aid is weaponized for geopolitical leverage.
Black South Africans are portrayed as passive beneficiaries of foreign aid, their agency erased while the US frames them as pawns in a diplomatic dispute over white Afrikaner rights.
The US government benefits, using aid leverage to advance geopolitical and racialized policy goals.
A six-year-old Ebola patient was taken from a DR Congo hospital by armed men amid community mistrust of health facilities. She was later found safe and receiving treatment, while health officials blame misinformation for attacks on Ebola response teams.
The coverage centers on a child's survival and family separation, but subtly positions local mistrust as a barrier to containment, deflecting attention from colonial medical violence.
International health organizations and pharmaceutical companies benefit from outbreak control narrative.

More than 70 medics have been infected with Ebola in the DRC, with 17 dead and over 200 total deaths. The outbreak is spreading due to weakened healthcare infrastructure, displacement camps, and poor sanitation.
The story shows Black healthcare workers and displaced people as victims of a structural neglect that leaves them exposed and dying.

Deputy Prime Minister Santia Bradshaw, a cancer survivor, advocates for Barbados to ensure access to brand-name cancer drugs, not just generics, citing concerns over side effects and quality. She argues that Barbadians deserve the same medications available globally, drawing on her personal experience with treatment limitations. The debate arises during discussion of a new medical products bill that would create a regulatory authority.
Deputy Prime Minister Santia Bradshaw gives voice to Black Barbadians' struggle for equal access to brand-name cancer drugs, using her own survival to highlight systemic inequities.
Pharmaceutical companies controlling brand-name drug pricing and supply.

The article uses the World Cup as a lens to discuss the slow global response to an Ebola outbreak, noting aid cuts and misinformation. Black communities affected by the outbreak are not mentioned directly, reflecting a media bias that sidelines their experience.
Black communities are rendered invisible in this story, reduced to a backdrop of epidemiological risk with no human voices or lived experiences.
Global pharmaceutical corporations and wealthy nations prioritizing World Cup tourism.

At least 30 people have died in a camp for displaced people in eastern DR Congo with Ebola-like symptoms, but many refuse testing, hampering containment. Sanitation is severely limited, and deaths far exceed the usual rate, raising fears of undetected spread among the region's 5 million displaced.
The displaced Congolese emerge as a faceless statistic of Ebola deaths and refusals, their agency reduced to a public health obstacle.
International pharmaceutical companies gain from continued outbreak funding and vaccine trials.

One month after declaring an Ebola outbreak in the Democratic Republic of Congo, MSF warns that failures in surveillance, testing, and community engagement are allowing the disease to spread faster than the response. Insecurity and weak healthcare infrastructure in eastern provinces exacerbate the crisis, with confirmed cases likely underreported.
The Congolese are portrayed as helpless victims of a failing system, their suffering reduced to a statistic in a narrative of institutional neglect.
International pharmaceutical and mining corporations benefit from the instability.

The article argues that poverty creates qualitatively distinct health outcomes, not merely reduced access. It critiques the global pharmaceutical industry for prioritizing profit over human life, and highlights struggles for food sovereignty, viral sovereignty, and universal healthcare in Africa. Coverage includes Kenya's universal health coverage challenges and Somalia's famine amid conflict.
The story portrays Black and impoverished populations as biologically and psychologically reshaped by deprivation, their suffering a byproduct of global pharmaceutical profiteering and colonial legacies.
Global pharmaceutical corporations and private healthcare industries.

This article challenges the view that global health disparities are merely quantitative, arguing instead that extreme poverty creates a qualitatively different human existence. It contends that conditions like lack of clean water represent not just less access, but a distinct reality shaped by deliberate structural forces.
Presented as a human data point, the Global South's poor are reduced to epidemiological figures that hide colonial extraction and deliberate impoverishment behind quantitative gradients.
Wealthy nations and global pharmaceutical corporations.

Somalia faces a severe humanitarian crisis driven by drought, conflict, and funding cuts, with over six million people facing food insecurity and 1.88 million children acutely malnourished. The report treats the famine risk as a natural disaster rather than a product of historical and economic exploitation.
The coverage reduces Somali people to abstract numbers of malnourished children and food insecurity levels, stripping them of human context or structural causes.
International aid contractors and local elites benefit from ongoing crisis funding.

The article raises concerns about severe psychiatric side effects of the asthma drug Singulair in an 11-year-old. It questions the FDA's responsibility to communicate new safety information to the public after drug approval.
Black children are portrayed as vulnerable patients harmed by pharmaceutical negligence, implying they bear disproportionate risks from inadequately monitored drugs.
Pharmaceutical companies benefit from minimized liability and continued drug sales.

An analysis of national CAR T-cell therapy data reveals that Black patients receive this treatment at only 67% of the expected rate. These racial disparities highlight ongoing inequities in access to advanced medical therapies for Black communities.
Black patients are reduced to a percentage disparity in CAR T therapy access, implying systemic exclusion is a numerical problem rather than a human one.
Insurance companies and pharmaceutical corporations benefit from restricted access.

The article discusses how poorly designed random testing of vaccines slowed rollout and adaptation to virus variants, linking this to subprime unemployment. It implies a legacy of empire without directly addressing Black communities.
The coverage reduces Black communities to an abstract data point in vaccine testing failures, erasing their lived experience of systemic neglect.
Pharmaceutical companies and global health authorities.

The infographic discusses Canada's war on drugs, highlighting its failure and the disproportionate criminalization of poor, Black, and brown communities. It contrasts this with a more lenient response to the opioid crisis affecting middle-class whites. The piece argues that enforcement has inadvertently boosted gang profits while harming marginalized groups.
Black and brown citizens are mentioned only as marginalized victims of a failed drug war, implying they are collateral damage rather than full subjects of concern.
Gangs and cartels profit from ongoing prohibition and street-level enforcement.

The Commonwealth Fund overview of Brazil's health system highlights progress in coverage and outcomes but notes stark racial gaps: Black Brazilians have lower life expectancy and higher maternal mortality than whites. The piece treats these disparities as given data points without naming systemic racism or colonial legacy as root causes.
Black Brazilians are reduced to statistical disparities in life expectancy and maternal mortality, implying their health outcomes are a natural fact rather than a result of systemic neglect.
The Brazilian state and private healthcare industries benefit from maintaining an unequal two-tier system.

Ghana's Health Minister reaffirmed the country's commitment to health reforms driven by national priorities during a meeting with WHO's Regional Director. The discussion focused on expanding health insurance, making primary healthcare free, and boosting local medicine production to reduce external dependency.
Ghanaian officials are portrayed as proactive leaders taking control of their health priorities, a portrayal that implies agency and capability rather than helplessness or dependency.
The Ghanaian government and its citizens benefit most from this strengthened partnership.

The article reports that Black maternal mortality is rising in the United States while rates for other racial groups decline. The framing treats the disparity as a numerical trend rather than a consequence of structural racism and unequal access to care.
Statistics stand in for people when rising Black maternal death rates are presented without context of systemic racism or historical neglect.
Private and public healthcare systems avoid accountability for racial disparities.

The article covers the black maternal mortality crisis in the U.S., highlighting that Black women are three to four times more likely to die from pregnancy complications than white women. It features a doula and a mother who share their experiences and advice for navigating a healthcare system marked by racial disparities.
Black women are presented through alarming mortality statistics, but the story also follows their personal agency and cautious planning to navigate a biased system.
The U.S. healthcare industry profits from neglected maternal care.

The article highlights the growing attention on Black maternal health, focusing on high mortality rates and systemic neglect. It calls for policy changes and community support to address disparities. The piece emphasizes advocacy and awareness efforts.
Black mothers are centered as individuals facing preventable harm, and the coverage advocates for systemic change rather than blaming them for poor outcomes.

This scientific article discusses integrating anti-racism into research practices by co-creating recommendations with Black communities. It acknowledges structural inequality and the need for systemic change within healthcare and academic settings.
The research positions Black communities as active co-creators of solutions, emphasizing agency and partnership over deficits or pathology.
Academic and healthcare institutions seeking legitimacy through community collaboration.

The article discusses the need for culturally competent substance use treatment for Black communities, emphasizing diversity, intersectionality, and the impact of racism and historical disparities on treatment outcomes.
Black people are presented as a diverse but underserved statistical group, defined by disparities in treatment access and outcomes.
Healthcare providers and pharmaceutical industries benefit from continued disparity-focused funding.

An Ebola outbreak in eastern Africa, driven by the rare Bundibugyo strain, threatens to become the worst ever due to lack of approved vaccines and treatments. Experts warn that international funding has slumped, and pharmaceutical companies have deprioritized this strain because it is rare and unprofitable.
Black communities in eastern Africa are portrayed as neglected victims of global pharmaceutical and funding priorities, their lives treated as expendable.
Big pharmaceutical companies benefit from ignoring rare strains.

Armed men stormed a hospital in Butembo, eastern DR Congo, taking a six-year-old Ebola patient and her mother. The attack reflects widespread distrust of Ebola treatment centers, which are often seen as foreign exploitation, complicating outbreak control.
Readers meet these communities as victims of both a deadly virus and misinformation, caught between life-saving treatment and local distrust fueled by colonial-era suspicions.
Global pharmaceutical companies benefit from vaccine development and future sales.

In Bunia, Democratic Republic of Congo, an Ebola outbreak has forced radical changes to traditional funeral rites, causing grief among families. Authorities work with communities to implement safe burial practices while struggling against misinformation.
The reporting humanizes the mourners by centering their grief and loss, but avoids deeper discussion of colonial-era neglect that weakened health systems.
International health organizations and pharmaceutical companies benefit from outbreak funding and vaccine contracts.

The article celebrates the recovery of Ebola patients in DR Congo, highlighting the joy and restored trust in healthcare. It also notes the challenges of overcoming local myths and misinformation that fuel violence against treatment centers.
Black Congolese are portrayed as resilient, faithful, and capable of recovery, yet their trust in healthcare is undermined by misinformation rooted in colonial legacies.
International health organizations and local authorities benefit from restored trust in Ebola treatment centers.

Resident doctors at LASUTH are on a three-day warning strike over unpaid allowances, promotion arrears, and poor working conditions. The Nigerian Medical Association warns that inaction could lead to wider healthcare disruptions.
The doctors are depicted as professionals whose legitimate grievances over pay and conditions are ignored, revealing systemic neglect that undermines Black healthcare workers.
The Lagos State Government benefits from delaying costs and wages.

Barbados minister Adrian Forde warns of young people abusing over-the-counter medications and prescription drugs, often mixed into a concoction called 'lean'. The new Barbados Medical Products Bill aims to regulate imports and sales, while a colleague highlights dangers from unregulated fade creams linked to a death in Jamaica.
Barbadian youth are portrayed as reckless drug abusers mixing over-the-counter medications into dangerous concoctions, implying a moral failing rather than addressing systemic neglect or limited mental health resources.
Pharmaceutical companies and unregulated importers benefit from weak enforcement.

A Barbados MP proposes that returning nationals pay for their own medications, arguing they never contributed to the national insurance system. The deputy prime minister resists the idea, focusing instead on improving healthcare delivery.
The MP depicts returning nationals as freeloaders draining public resources, implying Black diaspora members are undeserving and a burden on the state.
Barbados government and local taxpayers benefit from reduced healthcare costs.

The Barbados Ministry of Health and Wellness announced a fogging schedule for mosquito control in several parishes. The notice lists specific districts and instructions for residents, emphasizing operational details without addressing broader health disparities.
The fogging schedule presents Black communities as passive recipients of a public health measure, reducing their experiences to mapped zones and spray times.
Ministry of Health and Wellness, Barbados government.

Barbados's Ministry of Health reported two possible scarlet fever cases at a St Michael primary school, with the Chief Medical Officer urging calm. The story focuses on official response and disease facts, framing the incident as routine rather than alarming.
The coverage reduces Black Barbadian children to clinical cases and transmission risks, implying their health is a matter of administrative control rather than compassionate care.
The Ministry of Health and Wellness, which bolsters its credibility by minimizing public concern.

Hong Kong reports a rise in mpox cases linked to a gay-friendly sauna in Mong Kok, prompting health authorities to launch vaccination outreach. The story covers virus basics and prevention but does not address racial or structural inequalities.
Black communities are absent from this story, which reduces mpox to a public health update centered on a sauna-linked outbreak without addressing racial disparities.
Hong Kong health authorities benefit from targeted vaccination outreach to control spread.

The article reports on Ebola risks to Asia, emphasizing low probability but urging early detection. Africa is referenced solely as the outbreak's origin, with no discussion of local impacts or structural inequalities.
Africa appears as a geographic source of viral risk, with Black populations reduced to outbreak statistics and passive carriers of disease.
Global health security agencies and pharmaceutical companies preparing for future vaccine markets.

The article critiques global health disparities, arguing poverty produces distinct biological and psychological conditions. It highlights the prioritization of private profit over human life, with specific focus on Kenya's universal health coverage struggles, pharmaceutical industry exploitation, and food sovereignty movements in North Africa.
Poor and Black communities in Kenya and Africa are depicted as biologically reshaped by deprivation, victims of pharmaceutical profiteering and broken healthcare systems.
Global pharmaceutical corporations and private healthcare industries.

The article argues that prolonged poverty creates qualitatively different health realities for the global poor, not just lesser versions of wealthy health. It critiques the gradient model of inequality for masking how deprivation fundamentally restructures human life.
The global poor are depicted as biologically and psychologically altered by deprivation, their suffering framed as a structurally engineered condition rather than mere misfortune.
Global pharmaceutical and extraction industries that profit from unequal health systems.

Somalia's National Medicines Regulatory Authority and Egypt's Drug Authority signed a Memorandum of Understanding in Cairo to enhance cooperation on drug regulation and medical devices. The agreement focuses on knowledge exchange, data sharing, and capacity building for Somali technical staff, aiming to improve healthcare quality for Somali citizens.
Somalia is portrayed as a nation actively partnering to strengthen its healthcare system, emphasizing agency and capacity-building rather than dependency or victimhood.
Somalia's health regulatory agency and its public benefit.

The article reports that Black and minoritized ethnic communities in Canada face disproportionate negative outcomes in a specific area, likely health or social services. It relies on statistical data to highlight disparities but does not name racism explicitly as a cause.
Black and minoritized communities are reduced to data points in a study that documents disproportionate harm without exploring deeper structural causes.
Government agencies avoiding accountability for systemic health inequities.

Centres for Health and Healing promotes its private luxury rehab services outside Toronto, emphasizing personalized, holistic addiction and mental health care. The ad targets professionals but reflects a system where access to high-end recovery is commodified, potentially marginalizing Black communities who face structural inequality in healthcare.
Readers meet these communities as clients in a private, upscale rehab facility, implying that recovery is an individual journey available to those with resources, obscuring systemic barriers faced by Black Canadians.
Centres for Health and Healing, a private rehab corporation.

This web dossier traces alcohol production and consumption in Africa from pre-colonial times through the colonial and post-colonial eras, showing how alcohol became a marker of racial hierarchy and a tool for exploitation. It highlights how colonial regimes and apartheid in South Africa used alcohol profits to fund segregation while restricting Black access.
The historical role of alcohol as a tool of colonial segregation and economic extraction positions Black South Africans as a population deliberately targeted and exploited.
Colonial regimes, apartheid-era municipalities, and European brewing companies.

The report details how alcohol companies in sub-Saharan Africa, including South Africa, exploit weak regulations to expand market share, targeting communities with promotions and sponsorships while blocking public health policies. The Norwegian Fund's investments in these companies highlight how profit motives override health protections for Black populations.
Black South Africans are portrayed as targets of profit-driven alcohol industry tactics, with their health and safety subordinated to corporate interests and weak regulatory oversight.
Transnational alcohol companies and the Norwegian Government Pension Fund Global.

A new study reveals sub-Saharan Africa is failing to meet WHO alcohol reduction targets, with consumption rising due to aggressive industry expansion and weak policies. The region's high heavy episodic drinking rates highlight structural exploitation by Big Alcohol.
The story portrays Black communities in sub-Saharan Africa as vulnerable targets of Big Alcohol's calculated market expansion, implying systemic exploitation rather than individual failure.
Big Alcohol corporations

This story promotes the 988 Suicide and Crisis Lifeline as a free, confidential, and judgment-free mental health resource available 24/7. It emphasizes that the service is for everyone, including Spanish speakers through text and chat.
Black communities are portrayed as deserving of compassionate, confidential mental health support, with the service framed as universally accessible and free.

The article discusses a loneliness crisis among urban men aged 15-35, citing statistics on social isolation and mental health. It focuses on masculine norms and work pressure but does not address racial disparities or Black communities specifically.
Statistics stand in for people when the story cites loneliness rates and friendlessness percentages without any mention of Black men's specific experiences.
The tech and gig economy industries that profit from isolating urban work patterns.

The article discusses addiction in men through biological, social, and gendered lenses, citing statistics on substance use and treatment. It does not address racial disparities or systemic factors affecting Black communities.
Men are reduced to biological and statistical data on addiction, erasing the specific structural and racial contexts that shape Black men's substance use.
Rehab and pharmaceutical industries gain from pathologizing male addiction.

SMART Recovery offers evidence-based, stigma-free addiction recovery support through meetings, tools, and an app. The site emphasizes self-empowerment and multiple pathways to recovery, with no reference to race or structural inequality.
The content centers on individual empowerment and self-management, rendering Black communities invisible by omitting any mention of systemic barriers to recovery.
SMART Recovery organization benefits from broad appeal and partnership programs.

Maternal deaths in the U.S. declined overall in 2023, but Black women still died at more than three times the rate of white women. The article highlights widening racial disparities in maternal health but does not name racism as a cause.
Statistics stand in for people when Black maternal deaths are presented as a rate comparison devoid of the systemic neglect driving it.
Healthcare systems and insurers who avoid costly reforms.

The article reports that addressing Black maternal mortality could save thousands of lives and billions in healthcare costs and economic gains. It highlights that Black women are 3.5 times more likely to die in childbirth than white women, with preventable deaths persisting due to systemic inequities.
Black Americans appear here mainly as data points, with human lives reduced to cost-benefit calculations that frame their health solely as an economic problem.
Healthcare systems and insurers benefit from reduced costs.

The Minnesota Department of Health highlights a task force responding to a Congressional Black Caucus report on rising Black youth suicide rates. The story frames the crisis through a public health lens, focusing on systemic neglect but avoiding direct mention of anti-Black racism.
Black youth are presented as an at-risk demographic defined by suicide rates, their humanity reduced to a congressional report's alarming statistics.
The Minnesota Department of Health and public health institutions gain policy funding.

The article discusses how high inflation rates are negatively affecting mental health across the United States. It focuses on broad economic stress but does not explore the disproportionate impact on Black communities.
Black Americans are reduced to a data point in a generalized economic trend, ignoring how structural inequality amplifies inflationary harm in their communities.
Financial institutions and corporate landlords gain from inflation-driven profit margins.

Kenyan President Ruto defends a new Ebola facility amid local concerns, asserting that the government knows what it is doing. The story highlights tensions between international health interventions and local sovereignty in Kenya.
Kenyan citizens are portrayed as passive recipients of a foreign-designed Ebola facility, with their agency and local expertise sidelined in the headline.
International health organizations and foreign governments funding the facility.

A US doctor recovers from Ebola in Germany after being treated in Berlin, while the outbreak in the DRC surges to 488 cases and 86 deaths. The doctor's privileged access to experimental care contrasts sharply with the limited resources available to local populations.
Portrayed as passive victims without access to life-saving care, Congolese communities are reduced to a backdrop for a white doctor's recovery story.
Pharmaceutical companies testing experimental therapies benefit most from this outbreak.

The story covers Ebola outbreaks in Central Africa, focusing on tensions between health workers and local communities in the DRC and Kenya. It argues that vaccines alone are insufficient without trust-building and community engagement.
The article highlights community mistrust and the need for local leaders, portraying Black communities as active partners whose customs and fears matter.
Global health agencies and pharmaceutical companies gain most from managed outbreaks.

Amid a scarlet fever case at a Barbados primary school, virologist Dr. Camille Lange urges caution and transparency, noting parents feel their concerns are minimized. The story highlights a gap between official communication and community lived experience in a Black-majority nation.
Black Barbadian parents are framed as concerned citizens seeking transparency, their voices centered in a public health debate that treats them as legitimate stakeholders.
The Barbados Ministry of Health and Education benefits from caution that limits accountability.

Doctors and patients in Barbados are calling for new laws to allow kidney donations, citing 400 dialysis patients and rising non-communicable diseases. The story focuses on legislative needs rather than the structural inequalities driving the health crisis.
Barbadians appear primarily as a statistic of 400 dialysis patients, their suffering depersonalized while the systemic roots of kidney disease remain unexamined.

The WHO chief visited Uganda after an Ebola outbreak spread from the DRC. The story focuses on infection numbers and government response, with minimal attention to local community experiences or systemic vulnerabilities.
The coverage reduces Black communities in Uganda and the DRC to infection and death counts, stripping them of context and agency.
The World Health Organization gains legitimacy and global attention.

Health workers in DR Congo's Mongbwalu region fight an Ebola outbreak with little pay and rest. Poor living and working conditions in mining areas fuel transmission, while the WHO struggles to fund a $518 million response.
Congolese health workers are shown as under-compensated and overworked, their sacrifice highlighting the systemic neglect that exploits Black labor during crises.
The global gold mining industry benefits from cheap labor and weak health protections.

A Chinese medical team has arrived in the Democratic Republic of Congo to help contain an Ebola outbreak in a mining region where Beijing has significant mineral investments. The deployment is framed as filling a void left by the US, which has focused on travel restrictions and building a facility for its own personnel.
The Congolese population is rendered as a backdrop for geopolitical competition, their health crisis instrumentalized to highlight China's investment-driven diplomacy versus US isolationism.
Chinese mining and infrastructure corporations benefit from the conditions described.

WHO Director-General Tedros Adhanom Ghebreyesus visited Uganda after an Ebola outbreak spread from the DRC, with 19 confirmed cases and 2 deaths. The article focuses on case numbers and border screening, but lacks deeper context on the region's health infrastructure challenges.
The coverage reduces Black communities to case counts and death tolls, implying their suffering only matters as data points in a global health crisis.
Pharmaceutical companies gain from potential vaccine development contracts.

The webpage was inaccessible due to a security block, preventing analysis of its content. It appears to be a site about addiction statistics for African Americans.
African Americans are reduced to data points in addiction statistics, implying their substance use is a clinical problem detached from structural inequality.
Private addiction treatment centers benefit from framing addiction as an individual medical issue.

This study examines racial and ethnic disparities in alcohol-related mortality, noting that Black populations have higher death rates even when adjusting for consumption. The data-driven approach highlights unequal health outcomes but avoids exploring the structural factors such as targeted alcohol marketing and unequal healthcare access.
Black Americans appear here mainly as data points in a study that seeks to quantify mortality disparities without addressing the systemic causes driving them.
Alcohol industry benefits from framing as a consumption issue.

A NAADAC webinar highlights that Black individuals are half as likely to remit from substance use disorder as white counterparts despite more recovery attempts, pointing to medical mistrust and healthcare disparities. It advocates for racial literacy and recovery science to address these inequities.
Black people are primarily reduced to statistical disparities and systemic mistrust, implying their recovery struggles stem from medical bias rather than individual failure.
Healthcare systems and pharmaceutical companies benefit from perpetuating disparities without accountability.
The article examines how COVID-19 data revealed stark racial disparities, with African Americans dying at over double the rate of whites. It argues that pre-existing structural inequalities in health, housing, and employment were unmasked and worsened by the pandemic, calling for targeted policy action.
Black Americans appear here chiefly as numbers—disproportionate death rates and unemployment figures—rendering them a statistic of systemic failure rather than fully human.
Employers and corporations benefiting from a flexible, precarious labor pool.

The article discusses how the COVID-19 pandemic exposed deep healthcare inequalities affecting African Americans. It argues that systemic issues, not just the virus, drive worse outcomes for Black communities.
Black Americans appear here mainly as data points in a pandemic, highlighting systemic disparities without exploring the lived realities behind the numbers.
Healthcare systems and insurers benefit from maintaining cost-saving disparities.

The requested article about the Brazilian healthcare system could not be accessed due to a server error. No analysis of the content was possible.
The error message blocking access prevents any analysis of how Black Brazilians are portrayed in the healthcare discussion.

This themed issue explores relationships between public policy and health policy systems research through a policy capacity framework. It aims to fill a gap in knowledge about how policy capacity affects health system performance.
This story focuses on abstract policy capacity frameworks, with no specific portrayal of Black communities or their health realities.
Health policy researchers and academic journals.

Resident doctors in Nigeria threaten an industrial action over repeated assaults on healthcare workers, demanding better security. The story focuses on their collective response to workplace violence.
Nigerian resident doctors are portrayed as organized advocates demanding safety, highlighting systemic vulnerability in healthcare that disproportionately burdens Black professionals and patients.

The article reports that the Roxborough Hospital in Tobago will be fully operational by mid-November, nine months after its commissioning. It also details COVID-19 rental and food assistance provided to over 400 people, and notes Sinopharm is the most popular vaccine choice among Tobagonians.
Tobagonians emerge as a community actively served by government initiatives, with vaccine uptake portrayed as steady but cautious, avoiding victim or statistic reduction.
Government of Trinidad and Tobago benefits from showing public service delivery.

The WHO reports nearly 500 confirmed Ebola cases in Central Africa, with the outbreak spanning DR Congo and Uganda. The article warns the epidemic could rival the 2014 West Africa outbreak if strong interventions are not implemented.
The coverage reduces affected Black communities to case counts and death tolls, stripping them of context and implying passive victimhood without addressing systemic neglect.

The opinion piece argues that personalized medicine, using genetic data, can help close racial health disparities in the U.S. It acknowledges that these inequities stem from structural racism and calls for equitable access to new technologies.
Black Americans appear here mainly as beneficiaries of a medical innovation that could correct systemic health inequities through personalized genetics.
Pharmaceutical and biotech companies advancing personalized medicine.

The article compares U.S. and French responses to crack cocaine use, noting that in the U.S., the 1980s crack epidemic was framed as a criminal crisis affecting Black communities, leading to punitive policies rather than treatment. In France, racial data is banned, so crack use is viewed through a socioeconomic lens, though stigma still exists.
Black Americans are depicted as a threat driving a crisis, with their drug use framed as criminal behavior rather than a public health issue.
The U.S. criminal justice system and prison industrial complex.

The report exposes how the alcohol industry uses aggressive marketing and policy interference to undermine public health in Latin America and the Caribbean, targeting vulnerable groups like adolescents. Black communities are disproportionately harmed by rising alcohol consumption and related diseases, yet the industry's role in exacerbating structural inequalities remains unaddressed in mainstream discourse.
Black communities in the region are portrayed as passive victims of corporate manipulation, their health crises reduced to data points without agency or resistance.
Transnational alcohol corporations.

This article discusses the use of Massive Open Online Courses to train healthcare professionals in intercultural competence, focusing on Indigenous and prison health in Brazil. It argues that cultural diversity requires tailored health education to address systemic inequities.
Black and Indigenous populations in Brazil are portrayed as needing culturally adapted public health training through MOOCs, highlighting systemic neglect.
Brazil's Federal University of Rio Grande do Norte benefits from research funding and prestige.

Brazil's healthcare system is described as a dual public-private structure with notable successes in community health and social programs, though systemic challenges remain. The analysis focuses on economic opportunities and broad demographic trends without addressing racial inequities.
Black Brazilians are rendered invisible as the article discusses healthcare access and outcomes through broad national statistics and program achievements, erasing racial disparities.
Private healthcare investors and pharmaceutical companies benefit most.

The article discusses the strengths of school health models in Brazil, particularly in engaging families and promoting learning. It identifies opportunities for global school health but does not directly address racial inequities.
Black Brazilian communities are highlighted for their strengths in school health programs, yet the article overlooks how structural inequities limit these benefits.
Global health institutions and researchers.

The article highlights the disproportionate impact of the opioid crisis on Black communities, noting that despite similar drug use rates, Black individuals face higher arrest and incarceration rates due to the war on drugs. It calls for urgent, equitable action to address these disparities.
Black Americans are reduced to arrest and incarceration statistics in the overdose crisis, obscuring the human suffering and systemic roots of the epidemic.
Pharmaceutical companies profiting from opioid sales.

The opioid crisis disproportionately harms Black Americans due to historical racism, medical distrust, and biased pain management. The war on drugs and socioeconomic disparities further entrench addiction and limit access to treatment.
Black Americans are shown as victims of systemic neglect and medical bias, their suffering compounded by historical exploitation and inadequate institutional responses.
Pharmaceutical companies and the carceral system

The article links Black maternal mortality with the rise of Black-owned skincare companies, framing entrepreneurship as a response to healthcare disparities. It highlights resilience but does not deeply examine the structural racism in medical systems.
Black women are portrayed as resilient entrepreneurs, but the crisis of maternal mortality remains a statistical backdrop, downplaying systemic medical neglect.
Black-owned skincare companies and their investors.

The Canadian government announces a fund to support Black-led mental health projects addressing perinatal care, professional challenges for Black women, and food insecurity. These initiatives aim to create culturally appropriate resources and data to reduce systemic barriers.
Black Canadians are shown as active agents working to improve their own mental health through culturally focused initiatives, challenging deficit-based portrayals.
Black communities and the Public Health Agency of Canada.

The article details how Black communities in southeast Michigan face intensified mental health challenges due to pandemic aftershocks, federal funding cuts, and DEI policy rollbacks. It highlights the strain on local organizations and the eroding supports for uninsured individuals, students, and returning citizens.
Black communities are depicted as bearing the compounded weight of funding cuts, social upheaval, and policy rollbacks, struggling to access essential mental health care.
Federal and state governments cutting mental health funding benefit.

Black youth across Canada and the Caribbean face rising mental health issues but limited access to culturally competent care. Stigma and systemic neglect push them toward emergency interventions or isolation, while grassroots groups attempt to fill the gap.
Black youth are depicted as suffering in silence from systemic barriers and stigma, implying that their struggles result from neglected colonial and economic structures.
Governments and private healthcare systems avoid investment in culturally appropriate services.

Research from the University of Ottawa reveals over one-third of Canadians experience depression or anxiety, with Indigenous and racialized individuals 18 times more susceptible due to racism. The study calls for a national mental health plan with anti-racist, culturally sensitive care.
The study underscores Indigenous and racialized communities as victims of systemic racism, which exacerbates their mental health symptoms and highlights structural neglect.
Canadian governments and healthcare systems avoid accountability for systemic inequities.

The article reports that Black maternal mortality rates rose in 2023 despite an overall decline, highlighting preventable deaths and persistent racial disparities. It calls for amplifying Black women's voices and protecting Medicaid funding to address the crisis.
Black mothers are presented through alarming mortality statistics, which underscore systemic neglect but risk reducing their experiences to preventable data points.
Medicaid-dependent healthcare systems and insurance companies.

The article reports that the maternal mortality rate for non-Hispanic Black women rose slightly to 50.3 per 100,000 live births in 2023, showing no improvement. It highlights a persistent racial disparity but offers little analysis of underlying causes.
Numbers and trends define Black women's experience here, reducing a preventable crisis to a line on a graph without naming the systemic failures behind the data.
Hospitals and insurance companies benefit from inequitable maternal care.

The article reports a drop in confirmed Ebola cases in DR Congo due to better data, but highlights ongoing challenges like low contact tracing and community mistrust. It notes the outbreak occurs in a conflict-ridden region with no available vaccine for this rare strain.
The coverage reduces affected communities to numbers and failed contact tracing rates, implying their mistrust is an obstacle rather than a response to systemic neglect.
Global pharmaceutical companies benefit from the lack of a tailored vaccine.

The WHO and Africa CDC have launched a $518m plan to combat an Ebola outbreak in the DRC and Uganda, where cases and deaths are rising. The plan focuses on coordination and prevention, but local frustrations are growing over external interventions like a US quarantine station in Kenya.
The coverage reduces affected Black communities to case counts and death tolls, subtly implying their lives are valuable only as data points in a global health crisis.
Pharmaceutical companies developing vaccines and treatments for Ebola.

Scientists at Cambridge have successfully completed the first human trial of an AI-designed universal coronavirus vaccine, which could protect against multiple coronaviruses, including future threats. The vaccine was tested on 39 healthy volunteers and showed safety and broad immune responses. This technology aims to replace reactive vaccine development with a proactive, future-proof approach.
Black communities are largely invisible in this story, which centers on technological advancement and vaccine development without addressing racial disparities in access or trust.
DIOSynVax and the University of Cambridge benefit most from this research.
The WHO and Africa CDC have launched a 518-million-dollar plan to combat an Ebola outbreak in the DRC and Uganda. The plan focuses on coordination, surveillance, and community engagement, but lacks approved vaccines for the Bundibugyo strain.
Black communities appear primarily as passive bodies in need of international aid, overshadowing local expertise and agency in outbreak response.
International pharmaceutical companies seeking vaccine and treatment development opportunities.

Kanya King, MOBO Awards founder, gives her final interview before dying of colon cancer, urging Black communities to overcome stigma and demand early detection. She highlights health inequities like higher prostate cancer risk for Black men. Her message is one of strength through self-advocacy and community care.
Kanya King is portrayed as a fulfilled, purposeful leader whose final message centers on urgent health advocacy for Black communities, emphasizing resilience through self-care and early detection.
The UK healthcare system and cancer charities benefit from reduced late-stage diagnoses.
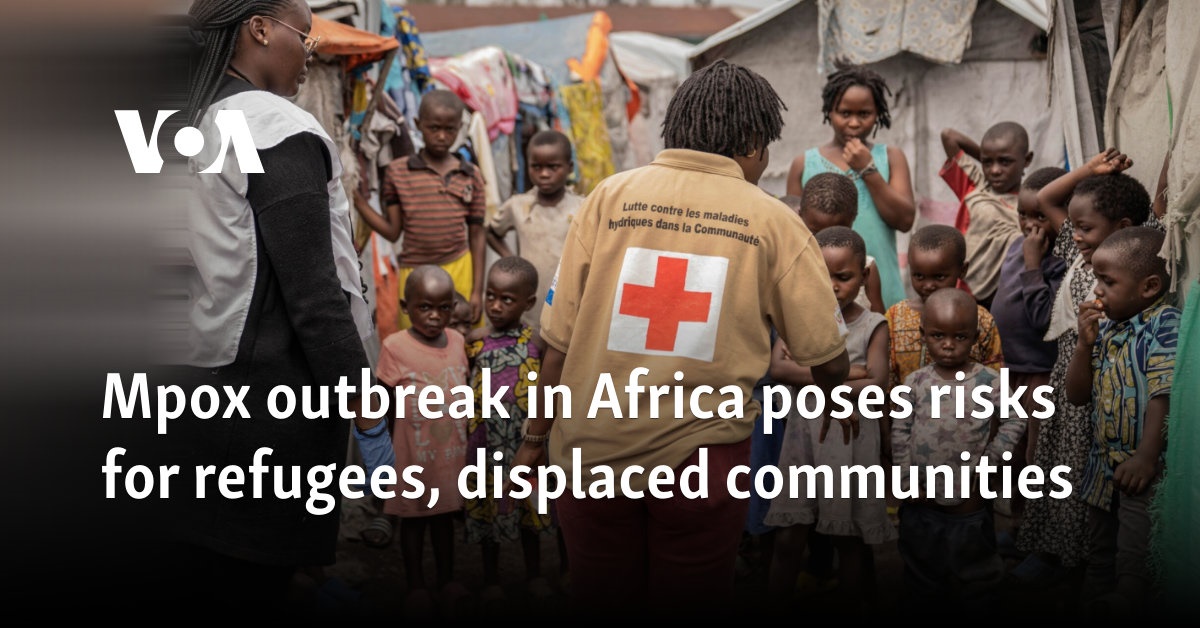
The article warns that mpox outbreaks in the Democratic Republic of Congo and neighboring countries pose severe risks for refugees and displaced communities, who cannot follow prevention measures due to overcrowding. UN agencies call for urgent international support to prevent the outbreak from becoming devastating.
The story depicts Black refugees and displaced people as helpless victims of disease and conflict, whose suffering is compounded by overcrowded living conditions and lack of international aid.
International pharmaceutical companies benefit from increased vaccine and treatment demand.

The African Development Bank has approved $33.64 million for Rwanda's Centre of Excellence for Biomedical Engineering and e-Health Project. The initiative aims to train students, upgrade facilities, and expand digital health tools, reducing reliance on imported medical solutions.
Rwandan citizens are portrayed as active participants in building their own healthcare future, with the investment highlighting agency and innovation rather than deficit or dependence.
African Development Bank and the Government of Rwanda.

The page is a generic drug interaction checker from Drugs.com, offering users a search tool to identify unsafe medication combinations. It contains no news content but rather a technical service page.
Black communities are reduced to a technical afterthought in a utilitarian tool that assumes neutral access, ignoring systemic medical neglect.
Pharmaceutical and tech companies that profit from data aggregation.

This article examines how alcohol affects women more severely than men due to biological differences, and notes rising drinking rates among women. It does not address how these trends or medical neglect disproportionately impact Black women.
Black women are statistically invisible in this piece, their specific health disparities erased by a gender-only lens that ignores racial differences.
Alcohol industry benefits from gender-targeted marketing.

This study surveys NGO alcohol and drug treatment services during COVID-19, focusing on operational disruptions and client needs. It does not disaggregate data by race, obscuring how colonial legacies and targeted marketing affect Black communities disproportionately.
Black Australians remain invisible in this study, which reduces a pandemic's impact on addiction services to survey numbers without naming how structural racism shapes access or outcomes.
Government agencies seeking cost-efficient data to justify funding cuts.

The UK government's Fingertips profile updates indicators on co-occurring substance misuse and mental health issues. The data is presented as neutral public health information, without acknowledging how systemic racism or colonial legacies shape these outcomes for Black communities.
Black communities are reduced to aggregated data points in official health statistics, implying their struggles are clinical problems without historical or social context.
The UK government benefits from depoliticized data that avoids structural accountability.

The article presents UK alcohol addiction statistics from official sources without breaking down data by race or ethnicity. This erases how structural inequality and targeted marketing disproportionately affect Black communities.
Black communities are rendered invisible as the data aggregates all demographics, masking how colonial legacies and economic stress heighten alcohol-related harm in Black neighborhoods.
The alcohol industry profits from normalized heavy drinking across the UK.

This article explores how stigma around substance use intersects with anti-Black racism. It highlights the structural inequalities that shape how Black communities experience and are treated for addiction.
Black communities are reduced to data points in a study about stigma, reinforcing the notion that their substance use is a public health problem to be managed.
The Institute of Alcohol Studies calls for a national strategy to reduce record alcohol harm in the UK, noting that deprived communities suffer disproportionately. The report proposes policy targets and public health measures but does not explicitly address how structural racism shapes alcohol-related outcomes for Black Britons.
Black communities vanish into statistical aggregates when this report discusses alcohol harm primarily through deprivation indices without naming racial disparities.
Alcohol industry profits from continued high consumption in deprived areas.

This article examines how commercial tobacco companies exploited post-Civil War racialized social structures to target Black communities, embedding health disparities within broader colonial legacies. It argues that current tobacco-related health inequities among Black populations are direct results of this systemic exploitation.
Black communities are depicted as populations historically targeted by tobacco corporations, highlighting systemic exploitation rooted in colonial-era racial hierarchies.
Tobacco industry corporations

The article ranks countries by alcoholism rates, with Mongolia and Eastern European nations topping the list. It presents the data as a neutral global comparison without examining systemic causes like economic exploitation or alcohol industry targeting.
The report reduces alcoholism to a ranked statistic, erasing the structural context of post-Soviet economic collapse and colonial disruption that drives rates.
Global alcohol industry escaping scrutiny for marketing in vulnerable regions.

The article explains the physical and psychological reasons alcohol is addictive, focusing on brain chemistry and emotional coping. It does not address how systemic factors like targeted marketing or historical inequities disproportionately affect Black populations.
The article generalizes addiction as a universal medical issue, erasing the specific ways alcohol industry marketing and historical trauma shape Black communities' higher addiction rates.
Alcohol industry profits from targeting marginalized communities.

The article examines how the War on Drugs disproportionately targeted Black communities, treating addiction as a criminal issue rather than a health crisis. It argues this legacy continues to harm African Americans through higher incarceration rates and limited access to treatment.
Black Americans here appear mainly as casualties of a racially targeted War on Drugs, their addiction portrayed as a punishment inflicted by the justice system.
Private prison corporations.
Anvisa's website outlines its role in monitoring health risks, registering new drugs, and cooperating internationally. The content is purely procedural and does not address racial disparities in health outcomes in Brazil.
Black Brazilians are invisible in this technical agency report, which presents health regulation as a neutral process, ignoring how systemic inequities shape access and outcomes.
Pharmaceutical corporations and international trade partners benefit from streamlined regulatory processes.

This webinar presents the 2025 UNODC World Drug Report's findings for Africa, focusing on shifting drug markets, trafficking routes, and consumption patterns. It emphasizes policy implications and public health responses while largely omitting the historical and economic exploitation affecting Black communities.
The webinar reduces African drug trends to epidemiological data and policy challenges, neglecting the structural violence and colonial roots shaping these patterns.
UNODC and international drug policy institutions benefit from framing the issue.
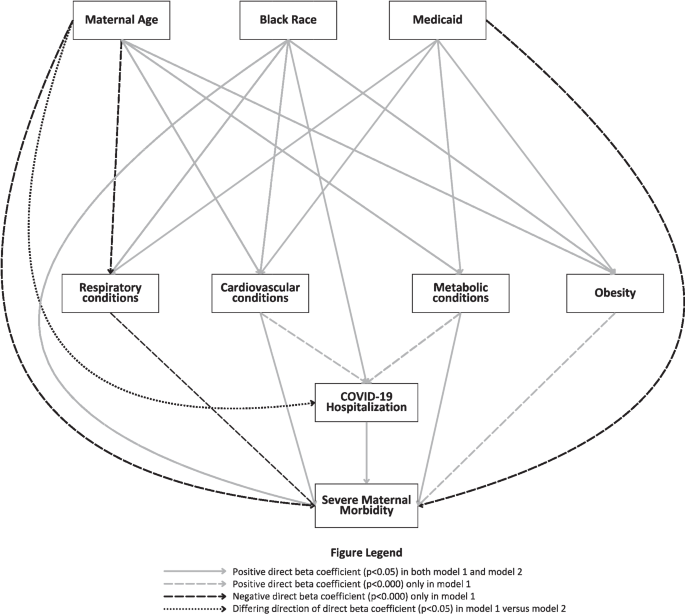
This study documents higher severe maternal morbidity among Black birthing people in New Jersey during COVID-19, exacerbated by physiological and healthcare access factors. The research calls for addressing both clinical care and structural inequities to reduce disparities.
Black birthing individuals are reduced to statistical disparities in severe maternal morbidity, implying their health outcomes stem from identity rather than systemic neglect.
Hospitals and insurers avoiding accountability for systemic failures.

This article presents mental health statistics showing Black Americans suffer disproportionately from anxiety, depression, and suicide yet rarely seek care. It links worsening conditions to funding cuts and economic pressures, urging community action to protect future generations.
Black Americans are reduced to a series of alarming statistics on mental illness and suicide, implying the crisis is individual failure rather than systemic neglect.
Private healthcare insurers profit when Black communities avoid costly mental health treatment.

This article by Crisis Text Line highlights the unique mental health challenges faced by Black, Indigenous, and People of Color during BIPOC Mental Health Month. It acknowledges systemic barriers but focuses on the organization's role in providing support services.
BIPOC communities are discussed primarily through the lens of statistical disparities, which implies their mental health struggles are a systemic pattern rather than individual failings.
Crisis Text Line benefits by positioning itself as a solution.

This is a listing for a VA healthcare system's addiction treatment center in South Dakota. It offers dual diagnosis services without mentioning race or structural context.
The content reduces Black veterans to a clinical category of 'addictive disorders' without any humanizing context, implying their struggles are merely medical or behavioral.
The VA healthcare system benefits from framing treatment as an individual problem.

The article examines how the War on Drugs has devastated Black and Latinx communities in New York through mass incarceration, job loss, and family disruption, while blocking their access to medical cannabis. It argues that current cannabis policies risk repeating racial inequities unless they explicitly address the harms of racist drug enforcement.
Black communities in New York are shown as victims of a drug war that fuels incarceration, poverty, and intergenerational harm while denying them medical cannabis access.
Pharmaceutical and corporate cannabis interests

Toronto Mayor Olivia Chow has proclaimed Black Mental Health Week, focusing on 'Joy as Resistance' to address anti-Black racism's mental health impacts. The week features community events and highlights systemic barriers to culturally responsive care.
Black Torontonians are portrayed as actively resisting systemic anti-Black racism through joy and collective healing, challenging deficit narratives that often dominate mental health discourse.
Toronto City Council and Black community organizations benefit from this framing.
The Canadian Minister of Mental Health and Addictions issued a statement for Black Mental Health Week 2025, emphasizing the theme 'Joy as Resistance' and the need for culturally appropriate mental health services. It highlights government funding for Black-led initiatives to address anti-Black racism and barriers to care.
Black Canadians are portrayed as actively resisting systemic oppression through collective joy, yet the government's framing risks reducing structural change to cultural celebration.
The Government of Canada benefits by appearing proactive on systemic racism.

The WHO reports that unsafe food causes 866 million illnesses and 1.5 million deaths annually worldwide, with young children at highest risk. The story highlights the disproportionate burden on Africa but frames the issue through statistics rather than systemic causes.
The coverage reduces African communities to mortality data and illness counts, implying their food safety crisis is a numerical problem without human depth.

Africa Check debunks a viral photo falsely claiming it shows Ebola patients arriving in Kenya from the U.S. The article clarifies the image is from a different context and warns against spreading health misinformation.
African communities are vulnerable to misleading health scares that exploit ignorance and fuel false crises not based on evidence.
Misinformation spreaders and sensationalist media outlets.

The article reports that as Sudan's war enters its fourth year, the UNFPA describes Khartoum as a ghost town with women bearing the heaviest burden. Thousands lack access to emergency obstetric care and gender-based violence services, with a $92 million funding gap remaining.
Sudanese women are depicted as war victims forced to carry their homeland's survival while facing catastrophic gaps in reproductive healthcare and protection.

The WHO reports improvements in the DR Congo Ebola outbreak but highlights ongoing challenges, including building community trust. Cases have dropped, but no vaccines or therapeutics are available yet, and clinical trials are being advanced. The WHO director calls for a ceasefire to allow humanitarian access.
The communities in this story are portrayed primarily through the lens of medical crisis and humanitarian need, emphasizing their vulnerability and the necessity of building trust.
WHO and international pharmaceutical companies benefit from advancing clinical trials and securing funding.

Health workers in eastern DR Congo use innovative Cubes and PPE to treat Ebola while facing shortages. The outbreak spreads due to delayed diagnosis and limited resources, highlighting systemic challenges in pandemic response.
Health workers and patients emerge as resourceful people managing a crisis, yet the coverage understates how colonial neglect and corporate extraction fuel systemic vulnerability to outbreaks.
International pharmaceutical companies benefit from limited local production of medical supplies.

Three new Ebola vaccines are being developed by IAVI, Moderna, and Oxford to combat the Bundibugyo species outbreak in the DR Congo and Uganda. Over 1,000 suspected cases and nearly 250 deaths have been reported, with concerns it could rival the 2014-16 West Africa outbreak.
Black communities in the DRC and Uganda are presented as numbers of cases and deaths, reducing their crisis to epidemiological data without humanizing their experience.
Pharmaceutical companies IAVI, Moderna, and Oxford gain from vaccine development funding.

Kenya protests a US-built Ebola quarantine facility for Americans on a military base, fearing it will import the disease. Health workers and citizens accuse the US of treating Kenya as a containment colony, while the government defends the project despite a court order.
Kenyans are depicted as disposable subjects in a colonial-style containment scheme, their safety disregarded to protect American lives elsewhere.
The United States government

East Africa faces a rapidly spreading Ebola epidemic caused by the rare Bundibugyo virus, with over 300 cases in DRC and Uganda. Conflict, funding cuts, and lack of an approved vaccine hamper the response, raising fears of a major crisis.
Statistics stand in for people when the outbreak is presented through case counts and death tallies, obscuring the lived humanity of affected Black communities.
Pharmaceutical companies fast-tracking vaccine trials.

Two people were shot dead in Nanyuki, Kenya during protests against a US plan to build an Ebola isolation center at a nearby military base. Demonstrators fear cross-border infection risks and have raised legal objections, while the US defends the facility as necessary for treating affected Americans.
The protesters are shown as reacting against a US medical facility that raises fears of colonial-style exploitation and health risks, framing their resistance as legitimate but costly.
The US government and its military-medical interests benefit from the isolation center plan.

A special report details how vaccine hesitancy in Sokoto, Nigeria, fuels the spread of circulating Vaccine-Derived Poliovirus, affecting children like Karima. The story highlights low routine immunization and community refusal but lacks analysis of historical distrust or economic constraints driving the hesitancy.
Portrayed as passive victims of a preventable disease, the community's vaccine refusal is blamed for the crisis, obscuring systemic failures like poverty and mistrust rooted in colonial medical exploitation.
Global pharmaceutical companies benefit from maintaining polio as a target for vaccine sales.

The article addresses Nigeria's maternal mortality and malnutrition crisis, highlighting policy goals and community-led solutions. It calls for sustained financing and implementation of nutrition interventions to save lives.
Statistics and policy goals dominate the portrayal of Nigerian women, reducing their lives to numbers while hinting at their resilience and systemic neglect.
The Nigerian government and international aid organizations.

Samantha James advocates for a national burn unit in Jamaica after a deadly explosion forces victims to seek expensive overseas treatment. She highlights how most families cannot afford medical evacuation, leading to preventable deaths like Dacia Forrester's.
Black Jamaicans are depicted as resourceful yet abandoned by systemic underinvestment, forced into desperate fundraising for life-saving care that wealthier nations take for granted.
Wealthy nations with burn centers and corporate sponsors benefit from medical tourism.

The WHO and PAHO certified Turks and Caicos Islands for eliminating mother-to-child transmission of HIV and hepatitis B. The milestone highlights strong health systems and equitable access, serving as a regional model.
Black communities in TCI are celebrated through health data, yet the achievement risks reducing their lived experience to a metric of system success.
The World Health Organization and Pan American Health Organization gain credibility.

PAHO warns of a measles surge ahead of the 2026 FIFA World Cup, with cases quadrupling in the Americas. The report emphasizes vaccination but does not address systemic barriers affecting Black and Indigenous communities.
Black communities in the Americas are rendered invisible in this alert, reduced to faceless case counts that obscure deeper structural inequities in vaccination access.
The global travel and tourism industry benefits from reassuring travelers.

CG Zest Wellness, a division of Coralisle Group Ltd., has launched a corporate wellness program in Barbados, offering health screenings, fitness events, and a wellness app. The initiative aims to promote healthier lifestyles and community wellbeing, building on a decade of similar programs in Bermuda, the Bahamas, and the Cayman Islands.
The story presents Barbadians as proactive participants in a corporate wellness initiative, highlighting agency and community engagement without pathologizing their health behaviors.
Coralisle Group Ltd. and its subsidiary CG United Insurance.

WaterAid's campaign reveals stark maternal health inequalities by examining what women pack for childbirth across 13 countries. In Malawi, women must bring their own razor blades and buckets due to lack of clean water and hygiene supplies, while UK mothers pack comfort items.
Black women in Malawi appear as victims of preventable harm, forced to improvise with razor blades and buckets, implying systemic neglect.
Private water and sanitation corporations.

Former Liverpool star John Barnes reveals he underwent prostate cancer surgery and urges men, especially Black men, to overcome stigma and get tested. He highlights that prostate cancer is more prevalent in Black men and calls for greater awareness.
Barnes speaks candidly about his diagnosis and recovery, positioning Black men as proactive agents in overcoming stigma and seeking life-saving care.
National health systems benefit from early detection and reduced treatment costs.

Kenya's health minister insists the US-funded Ebola quarantine center at Laikipia Air Base will open despite protests and court orders. Two people were killed in demonstrations against the facility, which critics see as a colonial-era imposition.
Kenyans are depicted as a population whose land and health security are subordinated to American needs, echoing colonial extraction.
The United States government

A Kenyan court extended a block on a US Ebola quarantine center in Nanyuki after protests left two dead. Kenyans accuse the US of offloading health risks, and the court ordered disclosure of the agreement with Washington.
Kenyans are shown as actively protesting and legally challenging a US quarantine facility, which highlights a community resisting perceived exploitation and health risks imposed by a foreign power.
United States government avoids domestic health risks and costs.

The WHO chief visits DR Congo as an aid group warns that four out of five Ebola contacts have gone untraced, suggesting the outbreak is larger than reported. The story highlights systemic failures in health infrastructure and community trust.
The report reduces Black communities to a count of untraced contacts and struggling health systems, implying their lives are expendable in the global health order.
Pharmaceutical companies and international health organizations gain from outbreak response contracts.

Hundreds of Kenyan youths protested the establishment of an Ebola quarantine center for US citizens at Laikipia Air Base. Health Minister Aden Duale claimed the facility was for everyone, not exclusively Americans, but the High Court had suspended its operation pending a legal challenge.
Kenyan youth appear as active resisters against a foreign quarantine plan, yet the coverage subtly questions their motives rather than the structural inequities driving it.
United States government and its disaster response infrastructure.

Former CDC head Tom Frieden warns that the world is failing the Ebola outbreak stress test, with underfunding and partial border closures hampering response. The story focuses on logistical and financial shortcomings without addressing colonial or economic roots of Africa's vulnerability.
Black African lives appear mainly as numbers—cases and funding gaps—while the systemic neglect of healthcare infrastructure remains unspoken.
Global pharmaceutical corporations benefit from underfunded public health systems.

A study by Fiocruz finds that 97% of pregnant Munduruku women in Brazil's Pará state have mercury levels four times above WHO safety limits, linked to illegal gold mining. The contamination passes to newborns, causing irreversible neurological damage and birth defects.
Indigenous Munduruku women are portrayed as victims of corporate extraction, their bodies measured in toxic levels while the root cause—illegal gold mining—remains background noise.
Illegal gold mining operations and the corporations that buy the mercury.

The African Union reports over 1,100 suspected Ebola cases in the DRC and Uganda, with 263 confirmed and 43 deaths. The outbreak, concentrated in Ituri province, is exacerbated by mining-related population movement and armed conflict, hindering response efforts.
Statistics and case counts dominate the coverage, reducing affected communities to data points while noting that over 60% of cases are women.
Mining corporations benefit from the continued labor flow in the region.

The article covers the plight of conflict-displaced people in the Democratic Republic of Congo who fear an Ebola outbreak would wipe them out due to lack of healthcare and safe shelter. It emphasizes the intersection of ongoing armed conflict, displacement, and the collapse of health infrastructure.
People in this story are presented as vulnerable and at imminent risk of extermination, reinforcing a narrative of helplessness in the face of structural neglect.

A study reveals that IMF lending conditions in West Africa reduce government health spending by roughly 6.2% annually. Binding policy reforms force austerity, limiting healthcare recruitment and investment, thus undermining universal health coverage.
West African nations appear as victims of external control, their health systems deliberately starved by IMF policies that prioritize financial stability over Black lives.
International Monetary Fund and global creditors.

A team led by ex-drug tsar David Nutt has developed a synthetic alcohol that produces a buzz without hangovers or severe drunkenness. While hailed as a potential solution to binge drinking, addiction specialists warn it could trigger dangerous cycles for alcoholics.
The coverage centers on addiction risk and scientific promise, yet Black communities are invisible in this discussion of synthetic alcohol despite facing disproportionate alcohol-related harm.
Imperial College London and the biotech industry gain from this synthetic-alcohol development.

The Telegraph's alcohol addiction section presents addiction primarily as a medical issue, with Black individuals often absent from humanizing stories. This framing obscures the role of structural inequality and targeted marketing in Black communities.
Readers encounter addiction through a clinical lens, reducing Black communities to data points without exploring the underlying social determinants.
Alcohol industry profits from continued consumption patterns.

This article reports a study identifying the exact amount of alcohol that raises blood pressure and heart disease risk. It presents findings as universal health guidance without discussing how structural inequalities or alcohol industry targeting affect Black communities disproportionately.
Readers encounter anonymous data without racial context, which can obscure how alcohol-related health risks are amplified by unequal access to healthcare and targeted marketing.
Alcohol industry benefits from depoliticized health advice that ignores targeted marketing.

The article compares U.S. and French responses to crack cocaine. In the U.S., media and policy framed crack use as a Black urban crisis, leading to criminalization, while France, lacking racial data, focuses on socioeconomic vulnerability and public health.
Black communities become a symbol of crisis and pathology, with their drug use criminalized rather than treated, reinforcing punitive stereotypes.
U.S. law enforcement and prison industry.

This study finds that rising inflation and Bank Rates during the cost-of-living crisis correlate with increased discrimination and poorer general and mental health for Black individuals in England. The research highlights how economic policies can exacerbate racial health inequalities.
By linking inflation and Bank Rates to worsened health and discrimination, the study presents Black individuals as data points whose suffering is economically quantified.
The Bank of England and financial institutions benefit from inflation policies.

The article reviews modern alcohol addiction treatments, including therapy, medication, and holistic methods, without addressing racial disparities in access or outcomes. It presents a one-size-fits-all approach that ignores how structural inequalities uniquely affect Black people.
Addiction treatment is presented as universally accessible and medically neutral, erasing how Black communities face unequal access due to cost, stigma, and systemic neglect.
Private treatment centers and pharmaceutical companies profit most.

This article details how addiction disproportionately harms African Americans due to the War on Drugs, unequal treatment access, and higher incarceration rates despite similar usage rates. It connects these disparities to systemic racism and ongoing civil unrest.
Numbers and disparities dominate the portrayal, reducing Black lives to percentages and arrest rates while the human cost of structural racism remains in the background.
The prison industrial complex and pharmaceutical companies gain from this inequity.

The article reports that African Americans drink less alcohol than white Americans but suffer more severe alcohol-related consequences. It mentions minority stress as a factor but primarily presents statistical comparisons.
Black Americans appear here mainly as epidemiological data points, their lived experience reduced to consumption rates and mortality figures without historical or systemic context.
Alcohol treatment and rehab industry.

The article critiques confrontational approaches to alcohol addiction treatment, arguing that breaking down psychological defenses can be harmful. It examines the rise and fall of this method without specifically addressing racial disparities.
Addiction treatment is discussed in clinical terms, abstracting the individual struggles that Black communities face, implying systemic disconnection from effective care.
Treatment industry professionals.
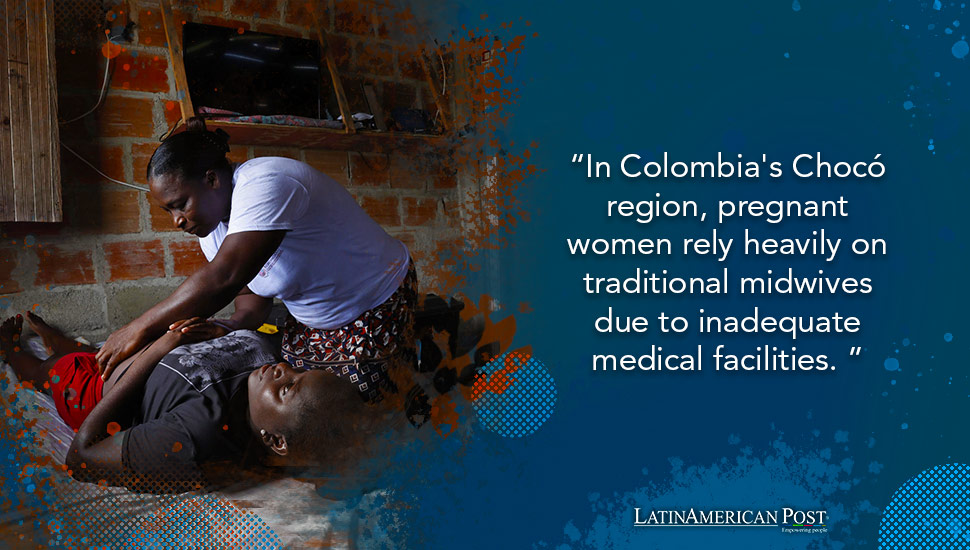
In Colombia's Chocó region, pregnant Black women rely on traditional midwives due to inadequate healthcare facilities marked by violence and neglect. Midwives work in dangerous conditions, yet their expertise is undervalued by a system that blames them for maternal deaths while failing to provide essential equipment or security.
Portrayed as resourceful yet abandoned, Black midwives and pregnant women embody resilience against state neglect that leaves them without basic medical facilities.
The Colombian government and extracted industries benefit from underfunded infrastructure in Chocó.

This interview discusses gender inequality in Brazilian women's health, focusing on adolescent pregnancy and limited access to public healthcare. It emphasizes economic rather than racial barriers, though structural inequality disproportionately affects Black women's reproductive autonomy and outcomes.
Black and poor Brazilian women appear as faceless data points on adolescent pregnancy and limited access to tertiary care, reducing lived experience to a clinical problem.
Private healthcare and pharmaceutical industries benefit from uneven public service gaps.

The article ranks countries by healthcare quality using global indexes, but ignores how race and colonialism shape access. It presents healthcare as a neutral comparison, obscuring structural barriers faced by Black populations.
Black communities are rendered invisible in this ranking, which reduces healthcare to a numerical abstraction without mentioning racial disparities or systemic inequalities.
International insurance companies selling expat health plans.

Ghana, led by President Mahama, spearheaded the Accra Reset initiative at the World Health Assembly, calling for a country-led, sovereign approach to global health reform. The high-level dialogue in Geneva focused on rethinking power dynamics and financing in global health delivery.
Ghanaian leadership is portrayed as proactive and sovereign, reframing global health reform as a matter of African agency rather than dependency.
Ghana's government and President Mahama's administration.

The article highlights the higher suicide rate among Black men compared to Black women, and offers practical solutions for mental health support. It points to cultural stigma and lack of access as barriers.
Suicide rates are foregrounded, rendering Black men as data points while obscuring the systemic factors behind the crisis.

The article explains the biological and psychological mechanisms of alcohol addiction, emphasizing the role of neurotransmitters and stress. It promotes professional treatment at Recovery Centers of America but omits any discussion of racial disparities or systemic factors affecting Black communities.
The clinical focus on brain chemistry and treatment options erases the social contexts of Black communities, where addiction is often rooted in systemic inequality and targeted alcohol marketing.
Recovery Centers of America and the private addiction treatment industry.

This article explains the science of alcohol addiction and offers prevention tips. It does not address how Black communities are targeted by alcohol advertising or face barriers to treatment.
The story presents addiction as a universal medical condition, erasing how Black communities face disproportionate alcohol-related harm due to targeted marketing and limited treatment access.
Alcohol industry profits from broad, undifferentiated consumer addiction narratives.
The article covers the Ebola outbreak in a remote gold mining town in the Democratic Republic of Congo, focusing on the surge of deaths and infections. It highlights the struggles of medical workers to contain the virus.
The reporting frames Congolese communities as a backdrop for medical failure, reducing human suffering to case counts and epidemiological metrics.
International pharmaceutical corporations and global health agencies.

The article examines Black maternal mortality in the U.S., attributing the crisis to structural racism, policy exclusion, and neglect of Black-led care. It argues that current policies often reinforce inequities and calls for a power shift to community-based solutions.
Readers meet Black women through alarming mortality statistics and policy critiques, but the framing reduces them to data points, obscuring individual humanity and lived experience.
The U.S. healthcare system and its dominant institutions maintain power and profit.

A March 2025 report from the National Center for Health Statistics shows the US maternal mortality rate for Black women was over three times higher than for other groups in 2023. The article presents the data without exploring the underlying structural causes.
Black women are reduced to a grim statistic, their deaths presented as a numerical disparity rather than a human tragedy demanding systemic change.
The for-profit healthcare system and insurance industry benefit from racial disparities.

The U.S. State Department issued an update on the Ebola response in Africa as of May 29, 2026, detailing containment efforts and international aid commitments. The report focuses on logistical coordination and funding allocations without mentioning local communities or systemic vulnerabilities.
Africans become depersonalized data points in a State Department update, their suffering reduced to progress metrics and response timelines.
U.S. pharmaceutical corporations and global health bureaucracies.

The article discusses how Africa and the world remain dangerously unprepared for future pandemics due to inadequate health infrastructure, economic disparities, and systemic neglect. It highlights the need for global cooperation and investment in public health systems to prevent catastrophic outcomes.
Africans are depicted as unprepared and vulnerable, reduced to a systemic weakness in global health security within a numerical risk analysis.
Global pharmaceutical corporations and wealthy nations.

The article argues that South Africa cannot end tuberculosis without addressing tobacco and nicotine addiction, which are major risk factors. It highlights the high rates of smoking and vaping in Black communities and links them to the country's TB burden.
The article reduces Black South Africans to statistics of TB cases and tobacco use, obscuring the systemic inequality driving these health disparities.
Tobacco and nicotine industries benefit from continued addiction in South Africa.

The WHO warns of a catastrophic Ebola outbreak in eastern DR Congo, worsened by armed conflict, displacement, and hunger. The Director-General pleads for a ceasefire to allow health workers to contain the fast-spreading virus.
The Congolese are depicted overwhelmingly as passive victims trapped between disease and violence, their agency erased by framing that centers international institutions as saviors.
International pharmaceutical companies gain from outbreak-driven vaccine and treatment contracts.

Kenya's High Court temporarily halted a U.S. plan to set up an Ebola quarantine facility for exposed Americans. The Law Society of Kenya and other groups opposed the proposal, citing health risks and arguing such facilities belong near outbreak epicenters.
Kenyans are portrayed as assertive actors defending their national sovereignty and public health against an outside power's risky proposal.
U.S. government benefits by avoiding quarantine on its soil.

The article critiques the U.S.-Uganda plan to contain Ebola, arguing it prioritizes Western containment strategies over local expertise and community needs. It highlights how structural inequalities and colonial legacies shape global health responses, often sidelining African nations.
Ugandans appear as passive recipients of a U.S.-led response, implying their agency is undermined by external control over their health crisis.
U.S. pharmaceutical and biodefense industries gain from shaping global health protocols.

A Kenyan court suspends a US plan to build an Ebola quarantine facility for American nationals in Kenya, amid backlash over secrecy and health risks. Activists and doctors argue the deal exploits Kenya and exposes its population to danger.
Kenya is cast as a convenient dumping ground for US health risks, implying Black lives are expendable in global power dynamics.
The United States government benefits by externalizing quarantine costs and risks.

The WHO chief visits Ituri as the DRC faces its 17th Ebola outbreak, with 121 confirmed cases and 246 suspected deaths. The Bundibugyo strain lacks approved treatments, and health workers struggle with scarce supplies amid public anger.
Readers meet these communities mainly as case counts and death tolls, depersonalizing the crisis and obscuring the human cost behind systemic neglect.
Pharmaceutical companies awaiting vaccine trials.

An Ebola outbreak in eastern DR Congo spreads undetected due to weak health surveillance and community mistrust, causing hundreds of suspected cases and deaths. Health officials struggle to catch up, while residents express fear and a need for protective measures.
The people in this story are portrayed as helpless victims of a deadly virus and systemic neglect, their deaths and fears reduced to a backdrop of institutional failure.
Gold mining corporations benefit from lax health monitoring in remote towns.

The article recounts the experiences of Ebola survivor Patrick Faley and other experts from West Africa's 2014 outbreak, drawing lessons for the current epidemic in DR Congo. It highlights the tension between public health measures and community practices, emphasizing speed, trust, and culturally sensitive engagement.
The story humanizes Black African communities through personal testimony, but it subtly centers Western expertise while framing local beliefs as obstacles to overcome.
Global health institutions like the WHO and international pharmaceutical companies.

The article details the challenges of containing an Ebola outbreak in DR Congo, caused by a rare species with no vaccine and set in a conflict zone. It focuses on health logistics and statistics, but provides little context on the structural inequalities shaping the crisis.
The outbreak is presented through clinical and epidemiological data, minimizing the lived realities of Congolese communities as victims of both disease and conflict.
The global health industry and pharmaceutical companies developing experimental treatments.

Scientists at Oxford University are developing an experimental Ebola vaccine targeting the Bundibugyo strain, with trials possible in two to three months. The outbreak in the Democratic Republic of Congo has led to 750 suspected cases and 177 deaths, and the WHO has raised the risk level to 'very high.'
The coverage reduces the outbreak to case counts and death tolls, rendering affected Congolese communities as passive data points in a global health narrative.
Pharmaceutical companies and research institutions gain from vaccine development and trials.
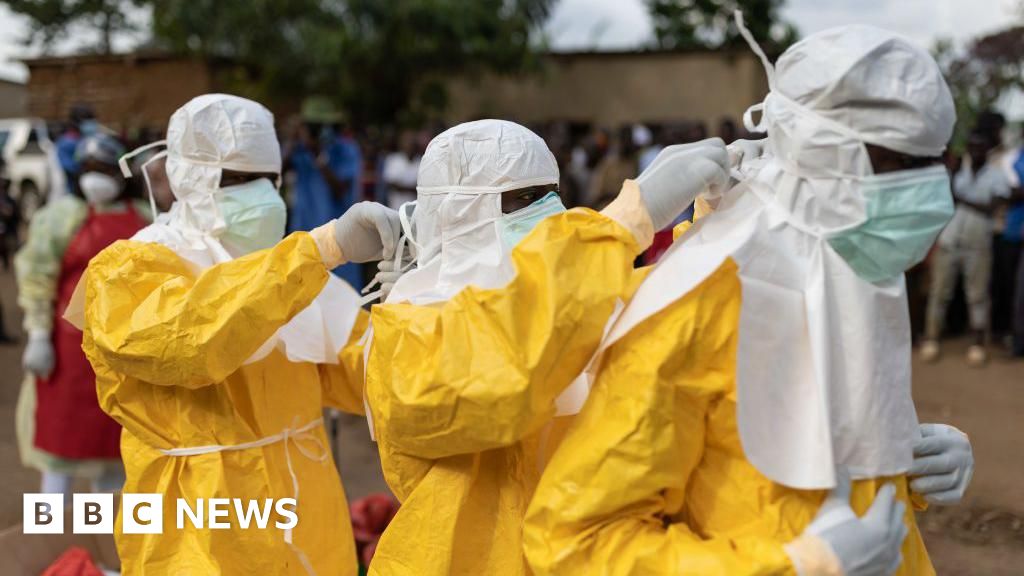
The BBC reports on a new Ebola outbreak in DR Congo caused by the rare Bundibugyo species, with nearly 250 suspected cases and 80 deaths. The article emphasizes the lack of approved vaccines and treatments, the challenges of civil war, and the threat to neighboring countries, but frames the crisis primarily through epidemiological data.
The outbreak is reduced to case counts and fatality rates, stripping Congolese communities of context and treating them as passive vectors of disease.
Global pharmaceutical companies gain from experimental vaccine and drug trials.

The article discusses how the Trump administration used the threat of Ebola to defend travel restrictions, framing the issue as a security matter. Black communities in Africa are portrayed mainly as vectors of disease, reinforcing stereotypes of the continent as a source of danger.
Africans are reduced to a health security threat in a travel ban debate, implying their lives matter less than Western safety.
The Trump administration benefits politically by appearing tough on immigration.

The WHO warns that conflict in DR Congo's Ituri province is crippling the Ebola response, with attacks on health workers and mass displacement worsening the outbreak. A rare strain of Ebola has caused 220 suspected deaths, and travel restrictions from Uganda, Canada, and the US further isolate the region.
Black communities in DR Congo are shown as passive victims of a dual catastrophe—Ebola and conflict—with little agency beyond awaiting external aid.
Armed groups and international pharmaceutical corporations benefit from instability and outbreak conditions.

A Kenyan court halted a US-planned Ebola quarantine facility for American citizens, citing public health risks. The decision followed local opposition and concerns about sovereignty and infection spread.
Black Kenyans are portrayed as passive subjects whose health sovereignty is overridden by a US facility designed to protect Americans, reinforcing colonial extraction patterns.
US government and its citizens.

A Kenyan court has temporarily blocked the opening of a U.S.-funded Ebola quarantine center, citing legal and transparency concerns. The ruling reflects tensions over foreign medical interventions in the region.
Kenyan communities are portrayed as legally pushing back against a U.S.-run quarantine center, asserting sovereignty and questioning foreign intervention.
U.S. military or health agencies seeking to manage regional outbreaks.
The Anambra State Government has ordered all mortuary operators to register or renew licenses by June 5, 2026, as part of health sector reforms. The move aims to improve monitoring, prevent illegal practices, and control disease outbreaks. Defaulters face sanctions under public health laws.
Black communities appear here as subjects of bureaucratic oversight, their health infrastructure framed through regulatory compliance rather than systemic neglect or exploitation.
Anambra State Government and its Ministry of Health.

Theresa Small's daughter Thalisa, born with a rare metabolic disorder, was denied vital medication by Queen Elizabeth Hospital in Barbados. After relocating to the US, Thalisa graduated from culinary school, showcasing personal success despite ongoing health challenges.
The story portrays a Black mother and daughter as resilient individuals overcoming systemic barriers, highlighting personal triumph over medical neglect and institutional indifference.
The Queen Elizabeth Hospital and Barbados government benefit from cost-saving medication denial.

The CEO of Queen Elizabeth Hospital in Barbados is advocating for a Caribbean network of hospital leaders to share best practices and accelerate healthcare transformation. He notes that geography and a lack of communication have hindered regional cooperation.
Clark is portrayed as a proactive leader seeking to overcome geographic and institutional barriers to foster regional healthcare collaboration in the Caribbean.
Caribbean hospital systems and their patients

The article commemorates the 25th anniversary of Barbados' National Wellbeing & HIV Commission, highlighting its role in HIV awareness, prevention, and support. It emphasizes community partnerships and a holistic approach to wellbeing beyond healthcare.
Black Barbadians are shown as agents of change and resilience, with the Commission celebrating their collective community effort to combat HIV stigma and improve wellbeing.
The National Wellbeing & HIV Commission and the Barbadian public.

Barbados has activated heightened surveillance and screening measures at ports of entry in response to an Ebola outbreak in Africa, though the risk to the island is considered low. Health authorities emphasize the country's preparedness and capacity to manage potential cases, drawing on lessons from the COVID-19 pandemic.
Barbados is shown as a capable state taking proactive steps to protect its population, with no stereotypes or pathologizing of Black communities.
The Barbados Ministry of Health and Wellness benefits from demonstrating preparedness and control.

Barbados President Jeffrey Bostic calls for community-level engagement and cultural adaptation to combat noncommunicable diseases, emphasizing early screening and education. He highlights the need to align health policies with local traditions rather than abandoning them.
The portrayal emphasizes community agency and cultural adaptation in fighting NCDs, positioning Black Barbadians as resilient subjects rather than passive victims of disease.
The Barbados government and public health system benefit from community-based disease management.

A Kenyan court halted a US plan to open an Ebola quarantine facility for American citizens in Kenya, citing public health risks. The Katiba Institute argued the facility posed grave dangers, and the court agreed to suspend operations pending a hearing.
Kenya's sovereignty appears subordinate to US interests, with Black Kenyans depicted as passive hosts bearing health risks for American citizens.
United States government

Uganda has closed its border with the Democratic Republic of Congo due to a surge in Ebola cases. The closure follows exposure of Ugandan health workers to the rare virus strain. The World Health Organization's guidelines were defied in the decision.
The story frames Black people as victims of a disease outbreak, implying a lack of control over their health and wellbeing. The narrative focuses on the disease rather than the social and economic conditions that contribute to its spread.
WHO and pharmaceutical companies.

Yulixa Toloza
The story frames Yulixa Toloza as a victim of an illegal cosmetic procedure, highlighting the risks and consequences of such actions. This framing implies that the victim's death is a result of her own actions
Beauty Láser corporation

A Kenyan court has blocked a US-built Ebola quarantine centre. The centre was intended to house Americans arriving from the Democratic Republic of Congo. This decision comes as the US faces criticism for not repatriating infected Americans.
Black people are framed as statistics in the context of the Ebola outbreak, with the story focusing on the quarantine centre and the US response. This framing implies a lack of agency and autonomy for Black communities in addressing their own health needs.
US government

The World Health Organization (WHO) has called for a ceasefire in conflict areas of the Democratic Republic of Congo to combat the current Ebola outbreak. The conflict is hindering access to affected regions and compromising disease control. The WHO director-general will visit the epicenter of the outbreak to oversee operations.
The story frames Black people as victims of the Ebola outbreak and the conflict in the Democratic Republic of Congo, highlighting the challenges they face in accessing healthcare. This framing implies a lack of agency and control over their own lives and health.
WHO benefits.

The Ebola outbreak in the Democratic Republic of Congo has led to over 900 suspected cases and 179 deaths. African countries are working together to contain the spread of the disease. The epidemic is concentrated in the Ituri province, which has mining activities and armed conflicts, making it difficult for medical teams to access the area.
The story frames Black people as victims of the Ebola outbreak, highlighting the challenges they face in accessing medical care due to armed conflicts and mining activities. This framing implies that Black people are vulnerable to health crises due to structural factors beyond their control.
Mining corporations.

The World Health Organization (WHO) has confirmed the first recovery of a patient with Ebola in the current outbreak in the Democratic Republic of Congo. The patient was discharged from the hospital after testing negative for the virus. The WHO has recorded 125 confirmed cases of Ebola in the country
The story frames Black people as victims of the Ebola outbreak
Pharmaceutical companies.

The World Drug Report 2025 highlights a rapidly evolving drug landscape in West and Central Africa
The story frames Black people in West and Central Africa as statistics
The high-level dialogue
The story frames Black people in West Africa as statistics and victims of the drug trade

Ghana is working towards achieving medical sovereignty, as stated by Dr. Grace Ayensu. The article aims to discuss Ghana's efforts in this regard, but the content is not available due to a server error. Ghana's goal of medical sovereignty could have significant implications for the country's healthcare system.
This story frames Black people as proactive agents working towards self-determination in the healthcare sector, implying a sense of autonomy and resistance against historical colonial and neo-colonial medical practices. The narrative highlights Ghana's efforts to challenge dominant global healthcare structures.
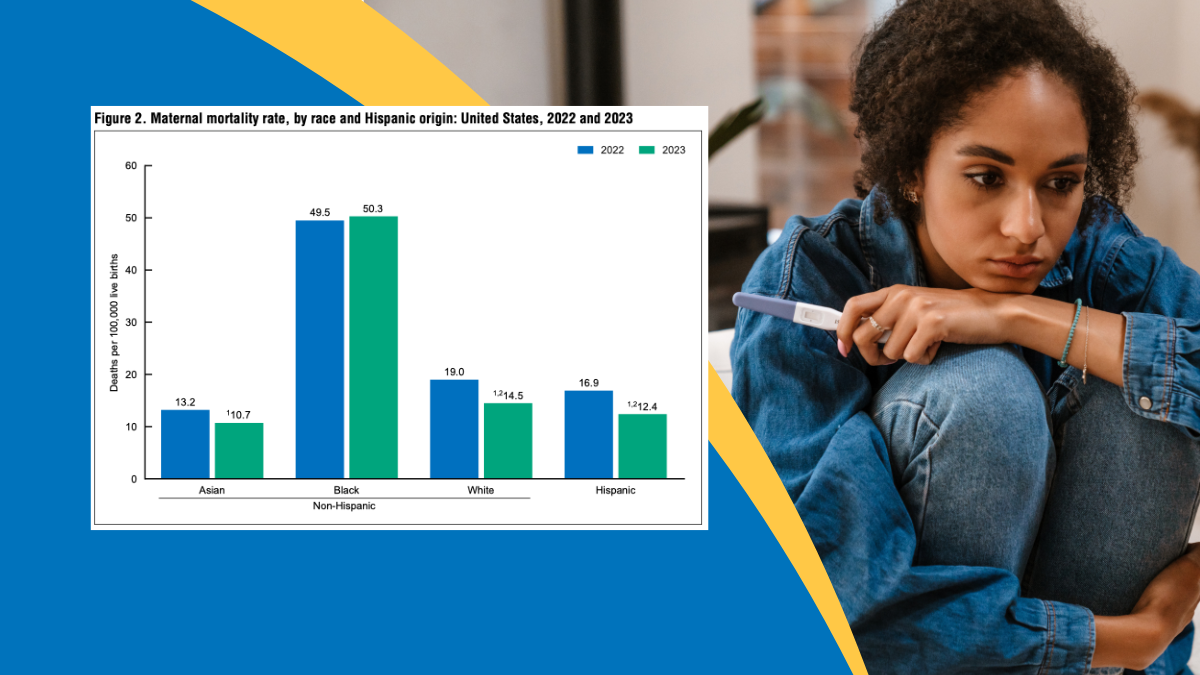
Maternal mortality rates in the US have declined
By focusing on statistics
US healthcare industry
The story highlights the racial disparities in the American healthcare system
Generally
Healthcare industry benefits.

The Mississippi State Department of Health's 2025 Maternal Mortality Report reveals that 83% of pregnancy-related deaths in Mississippi from 2017 to 2021 were preventable
Readers meet Black mothers as vulnerable victims of preventable deaths periodically.
Mississippi State Department of Health

The National Alliance on Mental Illness (NAMI) hosted a webinar discussing the impact of racism and trauma on Black mental health
Generally
NAMI benefits.

The article highlights the unique mental health challenges faced by Black people, including high rates of depression and suicidal thoughts. It discusses the need for culturally resonant strategies to manage stress and promote mental well-being. The article also introduces the
Readers meet Black communities as resilient yet vulnerable to mental health issues.
Mental health industry.

The study examines the pathways to recovery from alcohol use disorder in a Black community
Readers meet these communities as individuals recovering from alcohol use disorder.
Pharmaceutical companies.

The Canadian government has launched a renewed Canadian Drugs and Substances Strategy to address the overdose crisis
Notably absent is discussion of Black Canadians' specific struggles with substance use.
Canadian government

The article discusses the potential increase in alcohol consumption during the COVID-19 pandemic. It explores the possible reasons behind this trend and its implications for public health. However
Generally
Liquor industry

The COVID-19 pandemic has highlighted the need for a Just Recovery in South Africa
Black South Africans appear as needing a Just Recovery from COVID-19 now.
South African government.

The U.S. overdose epidemic is widening racial disparities
Black communities are portrayed as disproportionately affected by the overdose epidemic.
Pharmaceutical industry

The rate of drug overdose deaths among Black men in the US has risen sharply over the last decade
Black men are portrayed as struggling with addiction in rising numbers.
Pharmaceutical industry.

The study examines the relationship between racial discrimination and substance use disorders in the US
Black Americans are portrayed as struggling with substance use disorders due to racism.
Pharmaceutical industry

The United States has seen a significant increase in maternal mortality rates, with racial disparities persisting and behavioral health issues being a leading cause of maternal deaths during the COVID-19 pandemic. Maternal death rates are higher in states that haven't expanded Medicaid eligibility. The country's maternal mortality ratio remains higher than in comparable countries.
Racial disparities highlight Black mothers' struggles with healthcare access periodically.
Private insurance companies.

Racial disparities in maternal and infant health persist in the US
By focusing on statistics
Pharmaceutical industry

GRO Community
GRO Community portrays Black people as proactive agents of mental health change.
GRO Community

The mental health of Black youth is a silent crisis that is often a direct response to systemic inequities
Black youth appear vulnerable to systemic inequities affecting mental health.
Pharmaceutical industry.

The mental health crisis in Black America is being discussed, with a focus on systemic barriers that contribute to the issue. The crisis is affecting Black communities, and it's essential to address the root causes. Systemic barriers are a significant factor in the mental health crisis.
Black Americans are portrayed as vulnerable to systemic barriers affecting health.
Pharmaceutical industry

A new interview series is discussing the mental health crisis in the Black community
Black people appear as vulnerable individuals impacted by mental health issues.
Pharmaceutical industry.

The article discusses the barriers faced by individuals from Black and Asian backgrounds seeking support for alcohol addiction treatment. The drug and alcohol recovery support service BAC-IN explores these barriers and aims to provide more inclusive services. The article highlights the need for culturally sensitive support services to address the unique challenges faced by these communities.
Readers meet Black communities as facing barriers to addiction treatment services.
BAC-IN

The article reviews the best drug rehab centers in California
Black people are largely absent from this discussion of California rehab centers.
Rehab centers.

The article discusses rehab centers in Vancouver
Black people are largely absent from this Vancouver rehab center story.
Rehab centers benefit.

The Centers for Disease Control reports that excess alcohol use is the third leading cause of death from lifestyle-related factors in the US. Mountainside Drug Rehab and Alcohol Treatment Center offers comprehensive residential addiction treatment programs to address this issue. The center's team includes licensed and certified social workers
Black communities are notably absent from this addiction treatment discussion period
EPR Healthcare

The UK government has acquired investment to tackle drug dependence
Readers meet these communities as recipients of government aid and support services.
UK government

The city of Toronto has declared anti-Black racism a public health crisis
Black Canadians appear primarily as victims of systemic racism and discrimination.
Toronto city government.

The CDC reported that Black women have a significantly higher rate of maternal mortality
Black women are portrayed as disproportionately vulnerable to mortality during childbirth.
Pharmaceutical industry.

The article defines anti-Black racism in Canada as systemic issues within institutions like healthcare that perpetuate discrimination against Black-African Canadians, stemming from slavery and colonization. It highlights the negative impact on Black communities' health and calls for collaboration to eliminate these systemic barriers.
Black Canadians are portrayed as vulnerable to systemic racism and discrimination.
Canadian healthcare institutions.